Home » Recurrent Implantation Failure (RIF): Causes, Diagnosis, and Treatment Options
Recurrent Implantation Failure Treatment in India for Failed IVF Implantation

As a reproductive immunologist and fertility specialist, I understand that few experiences in the IVF journey are more disheartening than a failed cycle.
When this happens repeatedly, it leads to a condition we call Recurrent Implantation Failure, or RIF.
I am Dr. Jay Mehta, and at our dedicated Recurrent Implantation Failure (RIF) Clinic in Mumbai, my team and I focus on managing complex implantation challenges with a structured, scientific approach.
RIF is not a final diagnosis—it is a clinical situation that signals the need for deeper evaluation.
What is recurrent implantation failure?
Recurrent Implantation Failure (RIF) is a clinical condition where a patient fails to achieve a successful pregnancy after two or more consecutive embryo transfers.
This diagnosis is specifically applied when Top Quality Embryos (TQE) or genetically tested, chromosomally normal euploid embryos are used, and no other clear medical reason for the failure has been identified.
It is the "unexplained" gap between a perfect embryo and a successful pregnancy.
1. The Technical Definition vs. The Emotional Reality
While the medical definition requires two or more failures, we recognize that the journey of anxiety begins the moment the first IVF cycle fails.
Most patients enter IVF expecting success; when it doesn't happen, it creates a trauma that needs specialized attention.
2. The Search for "Fine Points".
As a dedicated RIF clinic in Mumbai, we don't just "try again." We look for the subtle details that may have been missed in previous standard IVF cycles:
-
Minor Anatomical Issues: Small polyps or filmy adhesions.
-
Hormonal Syncing: Misalignment between the embryo's age and the uterine lining's readiness.
-
Micro-inflammation: Silent infections in the uterine lining.
A careful, case-specific analysis is the only way to move from a generic "failure" to an individualized "success."
3. The "No Single Answer" Warning
Despite rapid advancements in reproductive science, it is often impossible to give one singular answer to every patient. RIF is usually a multifactorial puzzle.
Success comes from optimizing several small factors rather than looking for one "magic" reason.
4. The Role of Reproductive Immunology
This is one of the most misunderstood areas of RIF. While immunology is a powerful tool, it is often overused.
-
The 30% Rule: Out of every 100 patients we evaluate for RIF, only 30% actually warrant specialized immunotherapy.
-
Targeted Therapy: We warn against "blind" immunotherapy. We only use these treatments when specific diagnostic markers show that the mother's immune system is actively rejecting the embryo.
Expert Advice: RIF is not a dead end; it is a signal to stop and look closer. As a fertility expert, my job is to find those 'fine points' that standard protocols miss. We focus on truth and data, ensuring you only get the treatments you actually need.
What does RIF mean in IVF?
In the context of assisted reproduction, RIF stands for Recurrent Implantation Failure.
It is classified as a situation where a patient has experienced at least two failed attempts despite transferring high-potential embryos.
This classification is vital because these patients are technically expected to have the highest success rates.
When implantation does not occur despite good-quality treatment, it calls for a deeper, more technical evaluation of the case.
At our RIF clinic, we believe that identifying the exact cause can be complex and often requires looking beyond routine protocols to understand the subtle factors affecting implantation.
Patients must also understand that the age of the female partner is one of the most important diagnostic factors associated with implantation failure.
As female age increases, there is a definite reduction in oocyte (egg) quality, and consequently, the probability of forming genetically normal embryos reduces progressively over time.
Patient Tip: Understanding your embryo's status is the first step. If your embryos were not "Euploid" (genetically tested), the failure might be related to chromosomal issues rather than an implantation problem.
How many failed IVF cycles are considered RIF?
Technically, two or more failed IVF cycles involving TQE or euploid embryos qualify as RIF.
However, the emotional reality is often different. Many patients become extremely sensitive and anxious after even a single failed cycle, as they enter treatment with high expectations.
In India, a significant challenge is the lack of standardization. Many clinics lack advanced equipment; for instance, more than 85% of fertility clinics in India do not have the facilities for PGT-A (genetic testing).
Factors such as embryo freezing and thawing techniques can vary significantly between clinics, which may influence IVF outcomes.
At Shree IVF Clinic, Dr. Jay Mehta follows a detailed, case-by-case analysis of these technical aspects, helping us identify possible reasons in nearly 50% of recurrent implantation failure (RIF) cases we evaluate.
You can also watch our Embryo Freezing video to better understand how these laboratory processes impact embryo quality.
If you have experienced even a single failed cycle and feel uncertain about what happened, a technical protocol review can help assess whether your treatment followed international standards for embryo handling, freezing, and transfer.
Is recurrent implantation failure common in India?
Yes, Recurrent Implantation Failure (RIF) is becoming increasingly common, particularly as the average age of patients seeking fertility treatments in India continues to rise.
While it historically affected a smaller percentage of IVF patients, modern clinical data suggests that roughly 10% to 15% of women undergoing ART (Assisted Reproductive Technology) will experience RIF.
As you correctly identified, the shift toward "advanced maternal age" (37+) is the primary driver behind this trend, as both egg quality and uterine receptivity can change with age.
Why is Repeated Implantation Failure (RIF) on the Rise in India?
The increase in RIF diagnoses is a reflection of both biological realities and societal shifts in the last decade.
- The "Age 37" Threshold: By age 37, a woman’s ovarian reserve has decreased not only in quantity but also in quality. A higher percentage of embryos produced at this age are aneuploid (having an abnormal number of chromosomes), which is the leading cause of implantation failure.
- Late-Onset Lifestyle Factors: Factors such as sedentary lifestyles and increased prevalence of PCOS and endometriosis—which can worsen over time—frequently complicate the implantation environment for older patients. Early diagnosis of endometriosis and proper PCOS treatment can significantly improve reproductive outcomes.
- Increased Utilization: Because IVF is more accessible in India than ever before, the volume of patients has increased. Naturally, as the total number of IVF cycles goes up, the number of patients experiencing RIF also rises.
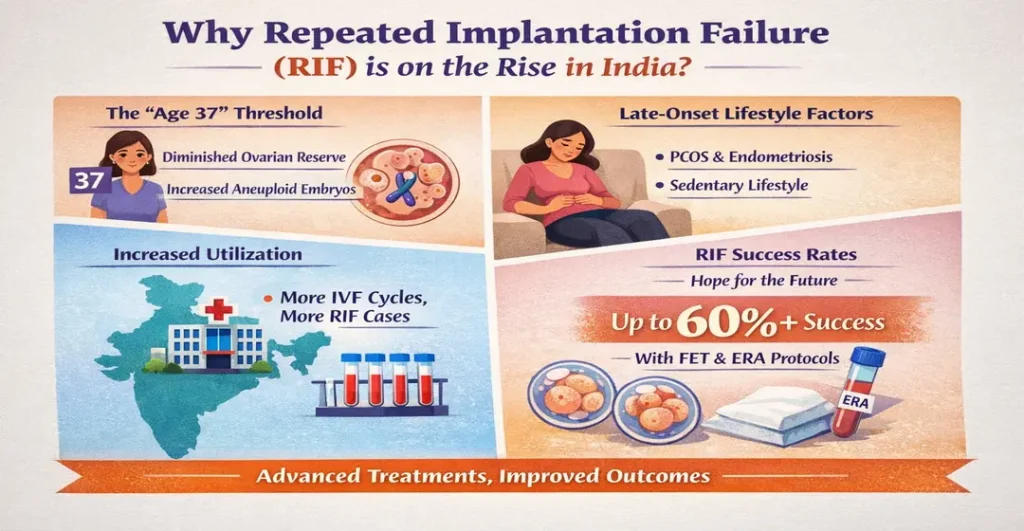
Repeated Implantation Failure Success Rates
Despite the rise in RIF cases, the outlook is far from bleak.
With personalized protocols—such as frozen embryo transfers (FET), which allow the body's hormones to reset, and ERA (Endometrial Receptivity Array)—the cumulative success rate for RIF patients often reaches 60% or higher over subsequent attempts.
Pro Tip: Don't lose heart due to your age. Precision medicine allows us to optimize "self-cycle" IVF even for patients in their late 30s by focusing on egg quality enhancement.
If you’ve experienced repeated failures, it’s time for a structured RIF evaluation—not just another cycle.
Consult Dr. Jay Mehta, one of the top implantation failure doctors in India, for a personalised implantation failure work-up and evidence-based fertility plan designed specifically for your age, ovarian reserve, and reproductive history.
Your next attempt should be smarter, not just repeated.
Is Recurrent Implantation Failure (RIF) a Diagnosis or Just a Description?
Dr. Jay Mehta classifies Recurrent Implantation Failure (RIF) as a description, not a final diagnosis.
Think of RIF as a clinical observation—a summary of what has happened (the failure of multiple high-quality embryos to implant) rather than an explanation of why it happened.
Classifying it as a description is vital because it shifts the focus toward a deeper medical investigation. Once the true underlying cause is identified, that becomes the actual diagnosis.
In the majority of cases, a deep technical understanding of reproductive medicine allows a specialist to pinpoint the specific culprit.
Once this diagnosis is firmly established and corrected, the path to a successful conception usually opens up.
In India, nearly 80% of IVF cycles are performed in clinics lacking advanced diagnostic equipment.
When patients transition to a facility with specialized tools, what was once an "unexplained" failure often becomes a treatable condition.
Common "true diagnoses" hidden behind the description of RIF include:
- Genetic Factors: Chromosomal abnormalities in the embryo.
- Uterine Receptivity: A displaced "window of implantation."
- Subtle Pathologies: Chronic endometritis or silent inflammation.
Don't settle for a description of failure when you can find a definitive cause.
If you have experienced multiple unsuccessful transfers, it is time for a deeper technical evaluation.
Connect with the leading recurrent implantation failure specialist in Mumbai, Dr. Jay Mehta, today for an advanced diagnostic review.
Take the next step toward converting your RIF diagnosis into a clear, personalized treatment plan focused on improving implantation success.
Does every RIF patient need reproductive immunology?
Reproductive immunology is a cornerstone of treating RIF, but it is often misunderstood.
As a specialist in this field, Dr. Jay Mehta warns against the "miracle cure" mentality. While science has advanced, there is rarely one singular answer for every patient.
In fact, out of every 100 patients evaluated for RIF, only about 30% actually require immunotherapy.
It is critical to avoid unnecessary treatments. We must distinguish between patients who truly have an immune-related implantation barrier and those whose failures are due to other "fine points" or minor technical details.
Scientific Tip: Immunotherapy is not a "one size fits all" solution. Ensure your specialist performs specific immunological marker tests before starting treatments like Intralipid Therapy or specialized injections.
What is a recurrent implantation failure Clinic?
A Recurrent Implantation Failure (RIF) clinic is a specialized fertility center designed to investigate why high-quality embryos fail to implant, focusing specifically on achieving a successful pregnancy using a couple’s own eggs and sperm (Self-Cycle IVF).
In India, these clinics serve as a vital alternative to the standard "one-size-fits-all" approach.
While many general fertility centers quickly pivot to donor programs after a single failure, a specialized recurrent implantation failure clinic uses advanced diagnostics to find a path to success without giving up on the couple's genetic link to their child.
Why is a Recurrent Implantation Failure clinic essential in Mumbai, India?
The efficiency of an RIF clinic stems from its commitment to "medical detective work" rather than moving immediately to the easiest solution (donor eggs).
- Moving Beyond the "Donor Default": In India, over 85% of couples are advised to switch to donor programs after just one or two failures. An RIF clinic challenges this trend by focusing on salvaging the couple's own biological chances.
- Specialist Evaluation: These clinics allow specialists to sit down with patients and evaluate the "most probable cause" of failure, whether it’s related to embryo genetics, uterine receptivity, or lifestyle factors.
- Access to Advanced Technology: Most standard clinics lack the equipment for complex procedures. An RIF clinic typically offers:
- PGT-A: To ensure embryos are chromosomally healthy.
- ERA (Endometrial Receptivity Array): To find the perfect timing for transfer.
- Immunotherapy & Hysteroscopy: To treat underlying uterine issues.
The primary mission of an RIF evaluation & treatment center is to empower educated patients who are not ready to abandon their dream of a genetically related child.
By providing a better perspective and a firmer diagnosis, these clinics transform "unexplained failure" into a strategic plan for a successful Self-Cycle IVF.
If you have been told that a donor program is your only option after a failed cycle, it’s time for a second opinion based on science, not shortcuts.
Book a consultation with our RIF specialists to explore how advanced diagnostics can help you achieve a successful self-cycle pregnancy.
Why Is Shree IVF Known as India’s First Recurrent Implantation Failure (RIF) Clinic?
Shree IVF Clinic Mumbai is India’s first dedicated Recurrent Implantation Failure (RIF) clinic, focused on helping couples who have faced multiple IVF failures—typically 2–4 unsuccessful cycles despite transferring high-quality embryos.
In 2023, we established India's first RIF Clinic to offer a dedicated OPD (both in-person and online).
What defines us as the "first" is our unique ability to provide world-class expertise to any couple in India, regardless of their location. Our model is built on three pillars:
- Predominantly Online OPD: We recognized that expert RIF advice shouldn't be limited by geography. By launching a dedicated online platform, we have already provided scientific guidance to over 3,000 couples across India.
- Effective Diagnosis Over Trial-and-Error: Most clinics repeat the same failed protocols. We focus on identifying the specific cause—the "fine points"—behind the failure to ensure the next transfer has the highest chance of success.
- Logistical Convenience: Our approach allows couples to undergo most of their treatment and monitoring in their own home city. You only need to travel to Mumbai for specific, advanced procedures, making the entire journey smoother and more cost-effective.
For many, the "first RIF clinic" represents a shift from "unexplained" hopelessness to "scientific" confidence.
By providing a firm diagnosis, we give couples the backup they need to pursue a self-cycle, even when they have previously been told that a donor program was their only option.
In just two years, this specialized focus has helped the majority of our patients address their underlying issues and finally achieve a successful conception.
Access the protocols of India’s first RIF clinic from anywhere in the country. Start your journey with a virtual consultation by calling 1800-268-4000 and get the scientific answers you've been searching for. Connect with an RIF Specialist, Dr. Jay Mehta, today.
Is one failed IVF cycle RIF?
No, a single failed IVF cycle is not considered Recurrent Implantation Failure (RIF).
Biologically, IVF is a complex process with many variables.
A single failure can happen due to a variety of factors and does not necessarily indicate an underlying chronic issue.
Medically, RIF is only considered when a patient has failed at least two or more embryo transfers with top-quality embryos, where no other detectable cause for failure is present.
In India, Dr. Jay Mehta, a fertility expert, notes that a significant "mushrooming" of small fertility clinics has led to several challenges for patients:
- Lack of Standardization: Many clinics operate without standardized techniques or high-end machinery, making it difficult to determine if a failure was due to biological factors or laboratory limitations.
- Exaggerated Promises: Discrete marketing practices often woo patients with false promises and inflated success rates. When these "exaggerated" expectations aren't met, patients are left without a clear scientific explanation for the failure.
- The Importance of Quality Control: For a failure to contribute toward a diagnosis of RIF, the embryos transferred must be of top quality. If the lab environment or egg/sperm handling is subpar, the failure may be a result of the clinic's processes rather than the patient's biological receptivity.
Pro Tips: One failure isn't the end—it's time for clarity."
If your first IVF cycle failed without a clear explanation, don't leave your second attempt to chance. Get a transparent, scientific review of your case from India's RIF specialists.
When should RIF be diagnosed?
A patient should only be labeled with RIF when two or more embryo transfers have failed under specific "ideal" conditions.
Because implantation is a complex biological event, diagnosing RIF prematurely can lead to unnecessary stress or a rush toward donor programs without exploring the true cause.
To reach an official diagnosis of RIF, a specialist must first ensure that the "basics" are handled perfectly.
The Three Criteria of a Repeated Implantation Failure RIF Diagnosis
For a failure to be classified as RIF, the following criteria should be met:
- Embryo Quality: The use of Top Quality Embryos (TQE) or, ideally, euploid embryos (those that have been genetically tested via PGT-A and confirmed to be chromosomally normal).
- Uterine Health: A pelvis that is confirmed to be free of obstructive diseases, such as fibroids, polyps, endometriosis, or adenomyosis.
- Absence of Known Causes: No other clear scientific reason for the failure can be identified through standard fertility testing.
The Future of Implantation Science
As Dr. Jay Mehta emphasizes, the science of implantation remains a medical "enigma." While we have mastered many aspects of IVF, the exact moment an embryo communicates with the uterine lining is still being decoded.
However, we are on the verge of a diagnostic revolution. Emerging fields such as proteomics, metabolomics, and transcriptomics are expected to transform how we treat RIF within the next decade, moving us from "unexplained failure" to "precision medicine."
Before labeling your journey as a failure, it is essential to rule out subtle physical barriers that standard ultrasounds might miss.
Expert Recommendation: Consider a 3D Saline Infusion Sonography (SIS). This advanced imaging technique allows specialists to rule out subtle uterine issues like small polyps, scarring, or a uterine septum that could be preventing your success.
5,550+
Google Reviews
416K+
subscribers
Is Repeated IVF Failure Always RIF?
No, repeated IVF failure is not always the same as Recurrent Implantation Failure (RIF).
While the terms are often used interchangeably, they represent two different clinical scenarios.
Most "repeated failures" are actually due to identifiable factors like maternal age, poor embryo quality, or untreated pelvic pathologies.
True RIF is a specific diagnosis reserved for patients who fail despite transferring high-quality, genetically normal (euploid) embryos into an apparently healthy uterus.
Why do IVF cycles fail even when the cause is "visible"?
In a vast majority of cases, IVF fails because of a specific, identifiable pathology.
When the cause is right in front of you, it is a repeated failure, not yet a RIF. Common visible causes include:
- Maternal Age: The single most significant factor affecting egg and embryo quality.
- Pelvic Pathologies: Identifiable conditions such as endometriosis, multiple fibroids, adenomyosis, or a chronically thin endometrium.
- Recurrent Poor Embryo Quality: Issues during the fertilization or development stage.
Dr. Jay Mehta emphasizes that once these pathologies are identified and treated with the necessary technical and surgical expertise, the path to conception usually becomes much smoother.
Patient Tip: If your IVF has failed, ask for a detailed "uterine environment mapping."
Conditions like fibroids, endometriosis, or adenomyosis may need treatment before the next embryo transfer. Consulting a specialist like Dr. Jay Mehta can help address the root cause and improve success chances.
Why are these pathologies often left untreated in India?
A common question from patients is, "If the pathology was visible, why wasn't it treated before my IVF?" The answer often lies in the infrastructure of the clinic.
Many fertility clinics that have "mushroomed" across India are standalone centers without a comprehensive hospital backup. They often lack:
1. Advanced Operating Theaters: The technical equipment needed to handle complex surgical cases like deep endometriosis or large fibroids.
2. Surgical Expertise: Many fertility specialists are not trained in advanced endoscopic surgery and rely on "ghost surgeons"—external consultants called in only for specific procedures.
This lack of integrated surgical care means that subtle but critical issues are often overlooked, leading to avoidable IVF failures.
Our clinic serves as a dedicated referral unit for fibroid patients across India. Because we possess both the advanced surgical theater and the technical diagnostic backup, we help patients differentiate between a failure caused by an untreated pathology and a true implantation enigma.
Expert Insight: If you have had a failed cycle, the first step is to determine if your previous clinic had the hospital backup to actually treat your underlying condition.
If they didn't, your "failure" might simply be an "untreated diagnosis."
When Does IVF Failure Become True RIF?
Recurrent Implantation Failure (RIF) is considered only after all identifiable or “visible” causes have been carefully evaluated and ruled out. It is not simply about multiple failed cycles—it is a diagnosis of exclusion.
To be classified as true RIF, the following criteria should typically be met:
- Frequency: More than two failed attempts at embryo transfer.
- Embryo Grade: The use of Top Quality Embryos (TQE) or, preferably, genetically tested euploid embryos.
- Uterine Environment: No detectable pelvic pathology such as fibroids, polyps, endometriosis, adenomyosis, or other structural abnormalities that could impair implantation.
Differentiating between repeated IVF failure and true RIF is the primary goal of a specialized RIF unit.
Understanding whether the failure is due to a treatable, visible cause or a more complex, invisible implantation issue fundamentally changes the treatment strategy and improves the chances of success in subsequent cycles.
Why Does Recurrent Implantation Failure Need Specialized Clinics?
Solving Recurrent Implantation Failure (RIF) requires more than just standard IVF; it requires a level of microscopic precision and infrastructure that is rarely found in general fertility centers.
At a super-specialized RIF clinic like Shree IVF Clinic, the focus is to identify the exact factor responsible for failure—whether it lies in the embryo, the uterus, or the laboratory environment—and address it with targeted, evidence-based technology.
Here is why a dedicated RIF center is essential for overcoming repeated failures:
In-House Surgical Expertise (The Pelvic Factor)
Many IVF failures are actually "untreated pathologies. " Conditions like fibroids, endometriosis, and adenomyosis require advanced laparoscopic surgery or hysteroscopic surgery before the next embryo transfer.
- The Gap: Most routine clinics in India are run by specialists who are not trained in advanced surgery. They often rely on "traveling" or "ghost" surgeons, which leads to fragmented care.
- The Specialized Advantage: A dedicated RIF clinic has an in-house, high-tech operating theater where surgeons can address these pelvic issues before the next transfer, ensuring a smooth path to implantation.
Full-Time Embryology & Advanced Lab Standards
The laboratory environment is the "womb" before the womb.
- The Gap: Over 80% of Indian clinics depend on freelancing or traveling embryologists who work in batches. This lack of a permanent, dedicated embryology team can compromise precision.
- The Specialized Advantage: An RIF clinic employs full-time, highly trained embryologists and utilizes advanced equipment like
- Time-Lapse Culture: Monitoring embryo development 24/7 without disturbing them.
- Embryo Biopsy (PGT-A): Checking the genetic health of the embryo.
- Advanced Oocyte Culture: Optimized techniques for egg handling to ensure the best embryo quality.
Ethical Reproductive Immunology
Immunology is a promising but often misused science in fertility.
- The Gap: Because many clinics aren't trained in RIF, they often "blindly" offer treatments like intralipids, plasma injections, or Lymphocyte Immunization Therapy (LIT) to every patient, even when not needed.
- The Specialized Advantage: Data shows that only 20% of RIF patients actually require immunological support. A specialized clinic uses honest, evidence-based testing to determine if these therapies are truly indicated, avoiding unnecessary costs and complications for the other 80%.
Transition from "Trial and Error" to Precision Medicine
A super-specialized RIF clinic incorporates all the necessary facilities—surgical, embryological, and immunological—under one roof.
This allows for a corrected diagnosis and an honest, ethical solution tailored to your best fertility potential.
Expert Insight: Don't settle for a clinic that "guesses" at your treatment. If you have experienced repeated failures, you deserve a facility that treats your case with the technical thoroughness it requires.
"Precision science, not random treatments." If you are being offered immunological injections or add-on therapies without a structured diagnosis, it may be time for a second opinion.
Why Routine IVF Clinics Often Fail RIF Patients?
Routine IVF clinics often fail RIF patients because they are designed for "standard" cases rather than complex "technical audits."
Most centers lack the high-end diagnostic equipment necessary to investigate why top-quality embryos fail to implant.
Additionally, the high density of clinics in India creates an economic pressure where centers may hold onto complex cases they aren't equipped to handle, rather than referring them to a specialist.
Why doesn't my local clinic have the equipment for RIF?
Most fertility clinics are structured around a volume-based model, designed to manage straightforward infertility cases efficiently. However, Recurrent Implantation Failure (RIF) is not a routine condition—it requires advanced diagnostics, surgical precision, and high-end laboratory infrastructure.
However, as Dr. Jay Mehta—who has been in the industry for more than 13 years—notes, treating recurrent implantation failure requires a much higher level of technical sophistication.
Investigating the "fine points" of a failed transfer requires specific machinery and laboratory standards that are not financially viable for routine clinics.
When a clinic is built for simplicity and volume, it may lack the tools to deeply investigate genetic, immunological, or subtle uterine factors that prevent implantation.
💡Patient Tip: When interviewing a clinic after a failure, ask, "Do you have in-house facilities for PGT-A and advanced uterine mapping, or do you outsource these?" In-house expertise usually translates to better quality control.
The "Mushrooming" Effect: Why referrals are rare in India
In recent years, India has seen a rapid rise in small fertility clinics. This "mushrooming" has created intense competition.
- The Reality: Many decent clinics struggle to cover their high overhead costs. To survive, they often feel they cannot "let go" of any patient—even when the case requires expertise or equipment they do not possess.
- The Result: Instead of referring a complex RIF case to a specialized unit, clinics may continue with "trial and error" cycles, leading to further failures for the couple.
Corporate Policies vs. Patient Justice: Why your doctor might not refer you
A ground reality in modern fertility care is the rise of large corporate IVF chains.
While these chains offer brand recognition, they often enforce strict internal policies that prevent doctors from referring patients to outside specialists—even if that specialist has the specific expertise the patient needs.
In these scenarios, the doctor may want to help, but corporate red tape forces them to keep the patient "in-system."
As a result, the patient—the end user—is the one who suffers. This is why Dr. Jay Mehta emphasizes the importance of choosing a specific doctor's expertise over a clinic's brand name or its proximity to your home.
Expertise vs. Proximity: Making the right choice
When you have experienced an implantation failure, the "convenience" of a clinic near your home should no longer be the priority. RIF is a technical enigma that requires a specialist's eye.
Dr. Jay Mehta’s practice functions as a referral unit precisely because we bridge the gap that routine clinics cannot. We focus on:
- Case Scrutiny: Reviewing the actual data from failed cycles—not just summaries.
- Independent Advice: We are not bound by corporate policies, allowing us to provide the most direct path to a Self-Cycle IVF success.
- Technical Depth: Access to high-end laboratory systems, surgical correction, and structured RIF protocols.
If you have experienced an IVF failure, the "convenient" choice is often not the "correct" choice.
Success in RIF cases requires a doctor who has the freedom to look beyond corporate KPIs and the technical backup to perform a deep dive into your biology.
Expert Insight: When dealing with RIF, you must choose a doctor of expertise rather than just a clinic close to your home. Your journey deserves a specialist who has the high-end equipment and the surgical skill to find the "fine points" that were previously missed.
"Don't choose a clinic based on distance—choose based on results."
If your previous cycles failed, it may be because your clinic lacked the high-end equipment or specialized protocols to handle RIF. Get the expert-driven care your case requires. Consult with an RIF Specialist Today. Call 1800-268-4000
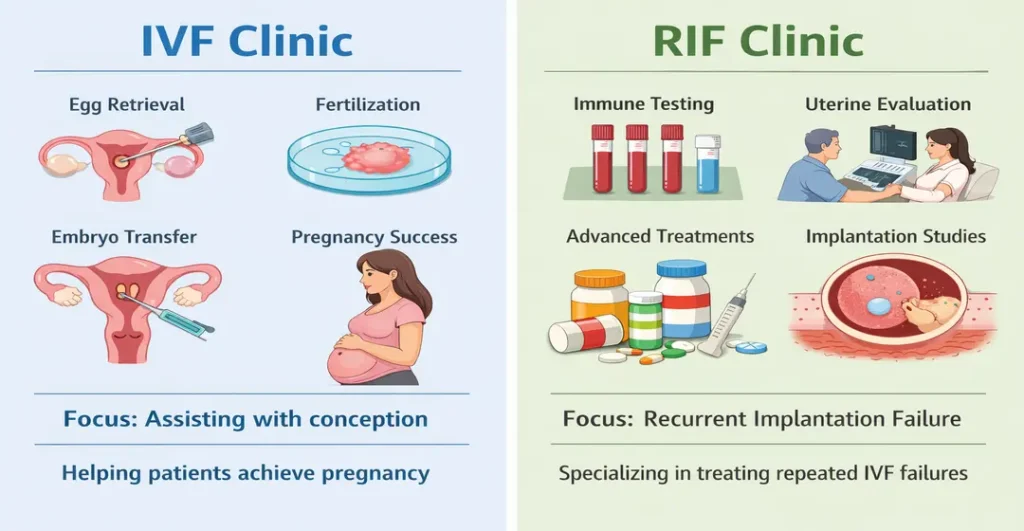
Difference between IVF clinic and RIF clinic
While a routine IVF clinic is equipped for standard fertility treatments, a Recurrent Implantation Failure (RIF) clinic is a "super-specialty" unit designed to solve complex cases where standard protocols have failed.
The difference lies in the level of technical investment, the depth of diagnostic machinery, and the specialized training required to address "invisible" barriers to pregnancy.
Understanding these differences is crucial for patients who have been told that their only remaining option is a donor program.
Scope and Regulatory Standing
In India, a routine IVF clinic (Level 2) is authorized to perform standard ART procedures such as Ovulation induction, Intrauterine Insemination (IUI), Basic IVF/ICSI, Treatment for blocked tubes, and Moderate male factor infertility
These clinics are optimized for what we may call “Level 1” fertility care—cases where the cause of infertility is identifiable and manageable with standard protocols.
Specialized RIF Clinic (Super-Specialty Unit)
A RIF clinic is designed for patients who have already undergone multiple failed embryo transfers despite good-quality embryos.
Its focus is not just on performing another cycle but on answering, "Why did implantation fail?" Is the issue embryonic, uterine, immunological, or laboratory-related? Can the self-cycle be optimized before considering donor options?
A RIF unit operates beyond routine IVF by addressing the subtle “fine points” often overlooked in high-volume settings.
Investment in High-End Technology
A specialized RIF clinic requires significant investment in advanced infrastructure that many routine clinics may not find financially viable.
| Feature | Routine IVF Clinic | Specialized RIF Clinic |
|---|---|---|
| Embryo Selection | Visual grading under a microscope | Time-Lapse Imaging and Spindle Assays |
| Genetics | Usually not offered in-house | PGT-A (Pre-implantation Genetic Testing) |
| Chromosomal Study | Rare | Non-invasive Chromosomal Studies |
| Uterine Analysis | Standard Ultrasound | ERA/EMMA/ALICE and 3D SIS |
| Immunology | Standard protocols | Immuno-modulation and Reproductive Immunology |
A routine IVF clinic helps couples conceive. A RIF clinic investigates why conception is not happening despite IVF.
If your case is straightforward, a routine IVF center is appropriate. If you are facing repeated failures, you need a super-specialized approach.
Because in complex fertility cases, the difference is not the number of cycles—it is the depth of investigation
Surgical and Immunological Expertise
Managing Recurrent Implantation Failure (RIF) requires advanced, super-specialized training that goes far beyond routine IVF protocols
- Immuno-modulation: This involves complex training in reproductive immunology to treat patients whose bodies may be "rejecting" the embryo. Unnecessary immune treatments can add cost and risk without benefit. A true RIF specialist knows who needs treatment—and who does not.
- Correction of Pathology: An RIF specialist is trained to identify and correct “fine-point” factors such as occult adenomyosis, subtle endometriosis, thin or displaced endometrium, previous surgical trauma, micro-adhesions, and transfer technique issues.
These are often missed in routine high-volume settings.
The “Donor Cycle” Default: A Critical Difference
This is perhaps the most significant difference for the patient.
- The Routine Clinic Approach: Due to limited diagnostic depth or laboratory capability, many clinics may suggest moving to a donor egg or donor sperm program after one or two failed attempts.
This recommendation is often made before conducting a comprehensive RIF evaluation.
- The RIF Clinic Approach: We prioritize self-cycle IVF. Our goal is to use science to make your gametes work. We believe patients should exercise extreme caution before agreeing to donor gametes and should first seek a specialized opinion.
If you have experienced multiple implementation or IVF failures despite transferring excellent or even genetically tested embryos, you deserve more than repetition—you deserve a structured, scientific investigation.
At Shree IVF Clinic, the dedicated RIF unit led by Dr. Jay Mehta supports patients across Powai, Borivali, Thane, Ghatkopar, Vashi, Bandra, and Andheri, offering advanced surgical expertise, ethical reproductive immunology, high-end embryology infrastructure, structured RIF work-up protocols, and global online OPD consultations.
Our goal is to move your case beyond the label of “unexplained” and toward a clearly defined, evidence-based solution because in complex fertility cases, precision changes outcomes.
Why Fragmented Testing Worsens RIF Outcomes?
Fragmented testing—the process of performing random, uncoordinated, and often unindicated medical tests—is one of the biggest contributors to the mismanagement of recurrent implantation failure.
When patients are treated in routine clinics without structured RIF protocols, they are often subjected to a “scattergun” diagnostic approach—multiple expensive tests without a clear clinical roadmap.
This leads to expensive, unnecessary testing and the waste of precious financial resources before a sound medical strategy is ever established.
The Trap of "Unindicated" Testing and Therapy
In many routine fertility centers, the lack of a structured, stepwise diagnostic protocol leads to two major issues:
1. Expensive Over-Testing: Patients are asked to undergo high-cost tests that may have no direct clinical relevance to their specific implantation failure.
2. Unnecessary Immunotherapy: Because "immunology" has become a buzzword, some clinics provide advanced immunological therapies as a standard "add-on" rather than a targeted treatment.
According to Dr. Jay Mehta, many such therapies in India are offered through informal collaborations where the consultant may not specialize in the nuances of implantation biology.
This leads to wasteful expenditure without improving pregnancy outcomes.
Patient Tip: If a doctor suggests expensive tests like "NK Cell Activity" or "HLA Cross-match" right away, ask for the specific clinical indication. Testing should always follow a logical, stepwise ladder rather than being done all at once.
The Financial Strain of Mismanagement in India
In India, fertility treatments are almost entirely self-funded by the patient.
Mismanagement at the routine clinic level means that by the time a couple finally seeks out a true Recurrent Implantation Failure Specialist, their finances are often completely exhausted.
This financial drain is more than just a loss of money; it is a loss of opportunity.
When resources are spent on unscientific or unindicated "fragmented" tests, patients may no longer have the budget for the actual advanced procedures (like PGT-A or specific immunomodulation) that could have actually solved their problem.
Why a Dedicated RIF Clinic is the "Need of the Hour."
Recognizing this gap in the Indian healthcare system, Dr. Jay Mehta established India's first dedicated RIF unit in Mumbai. The goal was simple: provide a protocol-based approach that leads to an effective diagnosis while protecting the patient’s time and finances.
Our dedicated clinic offers a unique advantage:
- Stepwise Diagnostics: We only initiate testing that is scientifically warranted based on your specific history.
- Specialized Expertise: As a specialist in reproductive immunology, Dr. Jay Mehta ensures that immunotherapy is only used for the 30% of patients who actually require it.
- Financial Protection: By avoiding "fragmented" testing, we ensure your resources are used for treatments that have the highest probability of success.
Accessing Specialist Care via the Online RIF OPD
The beauty of our dedicated RIF system is its accessibility. We have already assisted more than 3,000 couples through their journey, and much of this is done through our Online OPD.
This allows couples across India to receive a world-class expert opinion without the physical and financial burden of traveling to Mumbai for every consultation.
You receive a structured diagnostic plan from the comfort of your home and only travel if a specific, high-end procedure is required.
| Feature | Fragmented Testing (Routine Clinic) | Protocol-Based Care (RIF Clinic) |
|---|---|---|
| Approach | Random, non-coordinated tests | Logical, stepwise diagnostics |
| Cost | High wasteful expenditure | Targeted, resource-efficient testing |
| Specialization | Generalist/External consultants | In-house RIF & Immunology expert |
| Convenience | Frequent clinic visits | Comprehensive Online OPD support |
Experience the relief of a clear plan. You can start your journey with our Online RIF Consultation today to get a specialized roadmap without the need for immediate travel.
If you have faced repeated failures, don't let fragmented testing exhaust your hope or your savings. Our team in Mumbai is dedicated to providing the scientific backup and technical precision required to turn your RIF "description" into a successful "diagnosis."
What does a dedicated RIF clinic do differently?
A dedicated Recurrent Implantation Failure (RIF) clinic differs from a routine fertility center by moving beyond standard protocols to a granular, technical audit of every variable.
Instead of simply repeating a failed process, a specialized clinic investigates the "why" behind the failure by analyzing the sperm, egg quality, laboratory techniques, and the uterine environment with surgical precision.
Here is our Step-by-Step Approach to Complex RIF cases.
At our RIF clinic, the evaluation begins with a meticulous review of previous cycles. Dr. Jay Mehta and his team look at the case with a multi-layered approach:
1. Embryo & Lab Audit: We evaluate if the issue was related to sperm quality, egg (oocyte) quality, or specific development hurdles in the laboratory.
We check the precise grade of the embryos and whether genetic testing (PGT-A) for chromosomal normalcy (euploid status) was utilized.
2. Advanced Imaging: We look for missed pelvic pathologies. It is remarkably common in India for routine clinics to proceed with transfers despite the presence of fibroids, endometriosis, or adenomyosis.
A dedicated clinic identifies these and determines if surgical correction is required before the next attempt.
3. Endometrial Immune Profiling: If the embryos and pelvis appear normal, we perform a specialized biopsy to study microscopic implantation factors.
This includes testing for markers like MUM-1, uNK (uterine natural killer cells), IL-18, and BCL-6.
Patient Tip: If your previous clinic only looked at your "lining thickness" on a scan, you have only seen the surface. Ask for an endometrial immune profile to understand the microscopic environment where implantation actually happens.
4. Systemic Immunology: We move to advanced immunological testing, specifically looking at HLA matching and CDC cross-matching to see how the mother’s immune system reacts to the embryo.
Implementing Advanced "Correction" Techniques
Once the audit is complete, a specialized RIF clinic introduces high-end interventions that routine clinics may not offer. This may include:
- Oocyte Spindle Assay: To evaluate the metabolic health and structural integrity of the egg.
- Time-Lapse Imaging: Monitoring embryo growth in a stable, undisturbed environment.
- Protocol Refinement: Completely redesigning the stimulation protocol based on previous poor responses.
Are you tired of "copy-paste" treatment plans? Book a technical protocol review with Dr. Jay Mehta to see how advanced spindle assays or time-lapse imaging can change your results.
Managing Expectations: The Reality of RIF Science
Even with advanced scientific tools, implantation remains one of the great enigmas of reproductive medicine.
Success rates in complex RIF cases typically hover around 40–50%, even when everything is optimized.
Additionally, in 40% to 60% of cases, a definitive diagnosis remains elusive. Science is currently awaiting the commercial availability of advanced "omics"—transcriptomics, metabolomics, and proteomics—to solve the remaining mysteries of the womb.
However, a dedicated RIF clinic provides the maximum possible clarity available to modern science today.
Why "Switching to Donor" Isn't Always the Answer
In India, many patients are referred to RIF clinics after failing multiple cycles with their own eggs (self-cycle) and even failing 1–2 cycles with donor gametes.
It is crucial to understand that replacing the gametes (eggs/sperm) is not a treatment for RIF.
Many patients undergo donor cycles and still experience failure because the underlying implantation issue—whether immunological or uterine—was never addressed.
As the leader of one of India's largest RIF clinics, Dr. Jay Mehta focuses on solving the environment to make Self-Cycle IVF a reality whenever possible.
| The Routine Approach | The Dedicated RIF Clinic Approach |
|---|---|
| Repeats failed protocols | Performs a technical audit of lab & biology |
| Ignores "minor" fibroids or endo | Prioritizes surgical correction of pathologies |
| Quick jump to Donor Gametes | Focuses on Self-Cycle through immune profiling |
| Basic ultrasound monitoring | Advanced MUM-1, uNK, and HLA markers |
If you have experienced the heartbreak of a failed donor or self-cycle, it is time for a specialist's perspective.
Dr. Jay Mehta’s practice in Mumbai serves as a national referral point for complex RIF cases, offering the technical depth needed to find the "missed" factors.
Don't switch to a donor cycle out of frustration. Schedule a Self-Cycle Potential Assessment to see if advanced immune profiling can help you conceive with your own genetic material.
Why Is a Structured RIF Evaluation Important After Repeated IVF Failures?
When a couple faces repeated failures, the emotional and financial toll is immense.
The primary benefit of a structured Recurrent Implantation Failure (RIF) evaluation is that it shifts you away from guesswork and toward a concrete, scientific understanding of your specific situation.
Instead of jumping into a donor program out of frustration, you receive a clear roadmap that respects your genetic goals, your time, and your financial investment.
How Does Structured Evaluation Provide Diagnostic Clarity?
The most powerful advantage of a structured approach is understanding the “why” behind the failure.
- Reasonable Expectations: We provide a realistic outlook on your future treatment. Understanding the cause—or even knowing that the cause is currently an enigma—allows you to make informed decisions rather than emotional ones.
- Protecting Your Genetic Legacy: In India, many couples are pushed toward donor gametes prematurely. A structured evaluation often reveals that a "self-cycle" (using your own eggs and sperm) is still very much possible with the right technical adjustments.
- Avoiding Unscientific Therapy: Routine clinics often prescribe "blind" immunological treatments out of desperation. A structured evaluation filters out these unscientific, expensive, and potentially complicating therapies.
What Are the Realistic Outcomes of a Structured RIF Work-Up?
We believe in transparency. While a structured evaluation is the best path forward, we maintain total honesty regarding outcomes:
- The Diagnostic Reality: Approximately 40–60% of RIF cases may still be left without a definitive medical diagnosis because the science of implantation is still evolving.
- Concrete Guidance: Even without a single definitive cause, we can tell you exactly what the next best scientific step is to maximize your success probability—typically around 40–50% in complex RIF cases when optimized correctly.
Can You Access Expert RIF Care Without Traveling?
Yes, you can access expert care for Recurrent Implantation Failure (RIF) without traveling.
You shouldn't have to put your life on hold to get expert answers. Our clinic has pioneered a dedicated online model:
- Consult from Home: Most of our patients consult with us via online appointments. You don't need to leave your city, miss work, or arrange expensive travel just to get a world-class expert opinion.
- Comfort and Convenience: You only travel to Mumbai if a specific, high-tech procedure is required. The majority of your care and diagnostic planning happens in your comfort.
Stop guessing and start planning your next step with clarity. Get real answers—not just another IVF cycle.
Don't let an unexplained failure force you into a donor program. Access the structured protocols of India's leading RIF clinic from your home. Book Your Online RIF Consultation Call 1800-268-4000
Why Can’t Recurrent Implantation Failure (RIF) Be Treated with “Trial-and-Error IVF”?
Treating Recurrent Implantation Failure (RIF) with a "try it again and hope for the best" mindset is not only unscientific—it's a disservice to the patient.
In a country like India, where most fertility treatments are self-financed, a trial-and-error approach often leads to severe financial loss and emotional exhaustion before a true specialist is ever consulted.
Success in RIF is found in the "fine points" of technical precision, not in the repetition of failed protocols.
The Precision Approach: Finding the "Latching Point"
In many cases, the reason for implantation failure is actually straightforward if evaluated with technical expertise.
Dr. Jay Mehta emphasizes that by looking at specific "fine points," a specialist can usually identify a clear diagnosis. These points include:
- Cycle Monitoring: Precision in how the follicles and lining were tracked.
- Embryo Development: Analyzing the specific growth patterns and laboratory conditions during culture.
- Sperm & Pelvic Health: Identifying overlooked pathologies like fibroids, adenomyosis, or endometriosis.
Once we "latch upon" the correct pathology, we can offer a specific correction.
This allows the patient to undergo a targeted protocol rather than a random one, significantly increasing the likelihood of the desired outcome.
What Are the Risks of a Trial-and-Error Approach?
Because the science of human embryo implantation is still an "enigma" and continues to evolve, some clinics fill the knowledge gap with unproven or unnecessary treatments. Using a trial-and-error method often leads to:
- Unnecessary Medical Risks: Treatments such as immunological injections or add-ons may be used without a clear scientific indication
- Financial Exhaustion: In India, where most fertility treatments are self-financed, "trying everything" can deplete a couple's life savings before they find a solution that actually works.
- Emotional Distress: Repeated failures from "guessed" treatments lead to patients becoming grossly distended with the process, often giving up on their dream of parenthood entirely.
Why a Protocol-Based Approach is Essential?
A dedicated RIF clinic replaces "trial-and-error" with evidence-based medicine. Even though science doesn't have 100% of the answers yet, we utilize 45-50% of confirmed scientific data to optimize your chances.
This means only using advanced therapies—like immunomodulation or surgical correction—when the technical data supports it.
Dr. Jay Mehta’s philosophy is to protect the patient from wasteful expenditure by ensuring every step is purposeful.
In a country like India, this structured approach is the "need of the hour" to ensure couples don't lose their financial and emotional capacity to continue.
| Trial-and-Error IVF | Precision RIF Protocol |
|---|---|
| Guesswork based on "unexplained" failure | Identification of specific "fine points" and pathologies |
| High risk of unnecessary, expensive therapies | Targeted treatment (e.g., MUM-1, uNK markers) |
| Rapid financial and emotional burnout | Financial protection through indicated testing |
| Defaults to donor cycles quickly | Prioritizes Self-Cycle IVF through correction |
If you have been through multiple cycles that felt like "experiments," it is time for a specialist's intervention.
At our clinic in Mumbai, we specialize in auditing failed cycles to provide the clarity you deserve.
Don't spend your savings on "maybe." Use our Online RIF OPD to get a second opinion on your previous failures and receive a scientific roadmap that prioritizes your own eggs and sperm.
Don't switch to a donor cycle out of frustration. Schedule a Self-Cycle Potential Assessment to see if advanced immune profiling can help you conceive with your own genetic material.
What causes recurrent implantation failure?
Implantation remains one of the most complex processes in reproductive medicine—but we have moved beyond labeling repeated failure as simply “unexplained.”
Today, we understand that a successful pregnancy depends on a precise molecular "crosstalk" between a healthy embryo and a receptive uterine lining (endometrium).
When this dialogue fails repeatedly, we investigate the cause through three distinct layers.
1. Is the Problem the Embryo? (The Seed)
The first question an RIF specialist asks is, "Was the embryo genetically capable of producing a healthy pregnancy?"
- Euploid Embryos: A chromosomally normal embryo (euploid) is the gold standard. Even an embryo graded as “top quality” under a microscope may carry chromosomal abnormalities.
- The Crosstalk: A genetically normal embryo sends signals to the uterus. If the embryo is abnormal, the uterus may naturally prevent implantation to avoid an unhealthy pregnancy.
In many cases, repeated failure occurs simply because genetically abnormal embryos were transferred unknowingly.
2. Is the Uterus or Pelvis the Issue? (The Soil)
If the embryo is healthy but fails to stick, we look for physical or microscopic barriers in the pelvis.
- Visible Pathologies: Common causes in India include fibroids, endometriosis, adenomyosis, or an idiopathic thin endometrium.
- Microscopic & Inflammatory Factors: We perform a luteal phase guided hysteroscopy to look for "silent" issues. This includes testing for chronic endometritis using markers like MUM-1, uNK (uterine natural killer cells), BCL-6, and IL-18.
3. Could It Be an Immunological or Genetic Interaction Issue? (The System)
If embryos are euploid and the uterus appears structurally normal, we investigate how the maternal immune system interacts with the embryo
- HLA Typing: We check for human leukocyte antigen compatibility to see if the mother's immune system is overreacting to the embryo.
- Whole Exome Sequencing: A deep genetic dive to find the "right mix of genes" responsible for successful implantation.
Failed IVF vs. True RIF: Know the Difference
It is vital not to confuse a failed IVF cycle with recurrent implantation failure.
- Failed IVF: Often caused by poor egg/sperm quality, lab infrastructure issues, or unaddressed pelvic disease.
- True RIF: Occurs when two or more transfers of top-quality (preferably genetically tested) embryos fail in a healthy environment.
What If No Clear Cause Is Found?
As a specialized clinic, we provide a level of technical expertise not found in routine centers.
However, we maintain total honesty: even with advanced testing, a definitive answer is obtained in about 40–60% of cases.
For the remaining couples, we use the best available science to bridge the gap until future research in transcriptomics and proteomics provides the final pieces of the puzzle.
If you have "perfect" embryos that keep failing, it's time to look at the genetic and immunological crosstalk. Let India's leading RIF specialists find the missing link.
Accessing Expert RIF Care from Anywhere: Because the expertise required to treat RIF is not available across the country, we have pioneered an online RIF OPD.
This allows couples to interact with Dr. Jay Mehta, India's leading RIF specialist, and his team of specialists from the comfort of their homes.
Whether you are dealing with a single failed cycle or true recurrent failure, our protocol-based approach brings scientific clarity to your journey without the need for immediate travel to Mumbai.
Is RIF Caused by the Embryo or the Uterus?
Currently, the question of whether Recurrent Implantation Failure (RIF) is caused by the embryo or the uterus is one of the most debated topics in fertility science.
The truth is, implantation requires perfect coordination between both. In most cases, failure is not due to one single factor but a breakdown in the molecular dialogue between a competent embryo and a receptive endometrium.
However, in a clinical practice, we approach this by first "securing" the embryo quality so we can focus our investigation on the uterus.
Step 1: Is the Uterus the Primary Issue? (Preparing the “Soil ”)
Since the definition of RIF requires the use of top-quality or genetically tested (euploid) embryos, the uterus becomes the primary suspect in our investigation.
- The Importance of Hysteroscopy: A well-performed hysteroscopy is the gold standard for diagnosing uterine factors. It allows us to look past standard ultrasounds to find subtle issues in the lining that may prevent an embryo from "sticking."
- The "Hidden" Pathology: Many failures are caused by issues within the uterus that aren't visible to the naked eye, requiring microscopic or molecular evaluation.
Patient Tip: If you have had multiple failures, a standard ultrasound is not enough. A diagnostic hysteroscopy provides a 360-degree view of the "soil" to ensure it is ready for the "seed."
Step 2: Could the Embryo Still Be the Problem?
Even an embryo that looks "perfect" or is genetically normal (euploid) may have underlying issues that current technology cannot yet see. We use advanced laboratory machinery to bridge this gap:
- Time-Lapse Imaging:
Continuous monitoring of embryo development without removing it from the incubator. This allows embryologists to observe Precise cell division timing, Abnormal cleavage patterns, and subtle developmental delays
- Oocyte Spindle Assays:
Visualization of the egg’s internal spindle structure (its chromosomal division machinery) before fertilization. A disrupted spindle can affect embryo competence even if chromosomes appear normal later. In complex RIF cases, these “fine points” of embryology matter.
Step 3: Is the Issue in the Molecular Crosstalk? (The Frontier of RIF Science)
While we can check chromosomes and physical structures, the future of RIF lies in three emerging fields that study the "crosstalk" between the embryo and the endometrium.
While these are currently under investigation and not yet available for routine clinical testing in India, they represent the next decade of success:
| Field | What it Studies |
|---|---|
| Transcriptomics | The specific genes that must "turn on" for implantation to occur |
| Proteomics | The proteins secreted by the embryo and uterus to facilitate a bond |
| Metabolomics | The chemical constituents surrounding the embryo that signal its health |
Why Does Laboratory Infrastructure Matter in RIF?
When the reason for failure isn't visible on a scan, the "hidden problems" often lie in the technical handling of the cycle.
A Laboratory of Excellence equipped with advanced machinery is vital for RIF patients. Tools that are optional for routine patients become essential for those with repeated failures.
Repeated implantation failure is often solved not by doing “more IVF,” but by doing IVF with greater precision.
So, Is It the Embryo or the Uterus?
In a structured RIF evaluation, the answer is rarely simplistic.
-
If embryo genetics are compromised, then the embryo is the issue.
-
If uterine pathology exists, then the uterus is the issue.
-
If both appear normal, the problem may lie in their biological interaction.
The key is not choosing one side but systematically auditing both.
Dr. Jay Mehta’s technically upgraded IVF laboratory in Mumbai serves as a global referral point specifically because these advanced machines allow us to solve problems that routine clinics simply cannot diagnose.
Is your embryo's development being tracked with precision? Inquire about time-lapse embryo monitoring to ensure your embryos are developing in the most stable environment possible.
Differentiating Success: Expertise Over Routine
A technically upgraded laboratory is the backbone of RIF success. By integrating advanced imaging and specialized assays, we can offer hope to patients who have been unsuccessful elsewhere.
This technical depth is why Dr. Jay Mehta’s clinic sees patients from across the world who are seeking an answer to the "embryo vs. uterus" puzzle.
Why Is Recurrent Implantation Failure (RIF) Considered a Multifactorial Condition?
Recurrent Implantation Failure (RIF) is rarely caused by a single, isolated problem. Instead, it should be treated as a multi-diagnostic and multifactorial condition.
Because the "sticking" of an embryo involves a complex interaction between genetics, physical anatomy, and immunology, missing even one small detail can lead to repeated failure.
Approaching RIF this way allows us to provide concrete answers to you and your family, moving away from "bad luck" toward a structured scientific explanation.
1. Why Is a Stepwise, Multi-Layered Diagnosis Essential?
Because the causes are multifactorial, a specialized clinic investigates multiple layers simultaneously to find the specific combination of factors affecting your case:
- Embryo Factors: Chromosomal health, development speed, and metabolic markers.
- Uterine Factors: The presence of silent pathologies like fibroids, endometriosis, or adenomyosis.
- Molecular Factors: The microscopic "receptivity" markers in the uterine lining.
- Systemic Factors: The body's immune response and genetic compatibility between partners.
2. How Does a Multifactorial Approach Protect You from Wasteful Procedures?
In India, the lack of a multifactorial diagnosis often leads to two problematic extremes:
- The Donor Program Shortcut: You may be pushed toward donor eggs or sperm after a single failure. If the actual cause is uterine or immunological, switching gametes won't solve the problem, leading to further heartbreak.
- Unproven Immunotherapy: Many clinics recommend expensive "cocktails" like Lymphocyte Immunization Therapy (LIT) or intralipids out of desperation. Without a proven diagnosis, these are often wasteful expenditures with no clinical benefit.
3. How Does This Approach Help You Make Informed Decisions?
By identifying the specific "mix" of factors causing your RIF, we empower you to make sound clinical decisions.
Whether it requires a surgical correction, a change in lab technology, or a specific (and justified) immune treatment, the goal is always to maximize your Self-Cycle potential.
If you've been recommended to a donor program or LIT therapy without a clear reason, get a second opinion. Let's find out if a more precise, scientific approach can save your self-cycle.
Have You Been Advised to Do Donor Cycles or LIT Without a Clear Diagnosis?
If you’ve been recommended a donor program or immunotherapy without a structured explanation, seeking a second opinion may help clarify whether:
-
A correctable uterine issue was missed
-
Embryo competence was properly evaluated
-
Immunotherapy is truly indicated
Recurrent implantation failure is not a one-factor problem.
It requires a layered, technical, and individualized approach.
Precision diagnosis protects your biology, your finances, and your reproductive potential.
Why Is Recurrent Implantation Failure (RIF) Not Caused by a Single Problem?
Despite global advancements in reproductive medicine, the exact “moment of implantation” remains only partially understood. Implantation is a highly synchronized biological event requiring harmony between the embryo, the uterus, and the maternal immune system.
Because science is still evolving, a broad-spectrum evaluation is mandatory. This includes:
- Embryo Evaluation: Looking beyond grading to chromosomal health. An embryo that appears perfect under the microscope may still be genetically or metabolically compromised
- Uterine Evaluation: Ensuring the "soil" is receptive by assessing endometrial thickness and pattern, subtle cavity abnormalities, microscopic inflammation, and implantation window synchronization. Ultrasound alone is often insufficient in complex RIF cases.
- Overall Pelvic Health: Identifying missed pathologies. Even small, untreated pelvic abnormalities can disrupt implantation.
Even though a clear diagnosis is found in only 40% to 60% of cases, this protocol-driven approach is invaluable.
It provides a "technical audit" of what went wrong and, equally importantly, a list of what treatments will not work, preventing you from spending money needlessly on ineffective "trial-and-error" procedures.
Could a Silent Infection Be the Hidden Cause?
In India, one of the most frequently missed causes of RIF is Silent Endometrial Tuberculosis (Genital TB). Unlike pulmonary TB, this version often has no outward symptoms but causes:
- Severe Endometrial Fibrosis: Scarring of the uterine lining, making it difficult for the embryo to implant
- Reduced Receptivity: Permanent changes to the microscopic environment of the uterus.
This condition is often only discovered during a diagnostic hysteroscopy.
If your clinic has not performed a high-definition hysteroscopy to check the uterine factor, this silent pathology could be the reason behind repeated failures.
Before repeating another IVF cycle or moving toward a donor program, it is important to rule out silent pathologies that could be correctable.
Recurrent implantation failure is rarely due to a single problem—and solving it requires looking at every layer systematically rather than assuming it is simply “bad luck.”
What Are the Most Common Causes of RIF in Indian Patients?
In the Indian clinical context, the causes of recurrent implantation failure (RIF) are often multifactorial—influenced by delayed diagnosis, untreated pelvic conditions, prior infections, and region-specific health challenges.
While many cases remain "idiopathic" (where the exact cause remains unknown despite advanced testing), a specialized deep dive often reveals one or more underlying issues that standard IVF clinics may have overlooked.
Which Uterine Factors Commonly Cause RIF in India?
When a patient presents with RIF, we look for specific uterine and systemic factors that may have been overlooked during routine IVF cycles.
In India, the following conditions are the most common contributors.
- Thin Endometrium:
A uterine lining that fails to reach the optimal thickness (usually 7 mm or more) for implantation. This is often idiopathic or caused by previous infections or surgeries.
A thin lining is not just about thickness—it also reflects receptivity and vascular health.
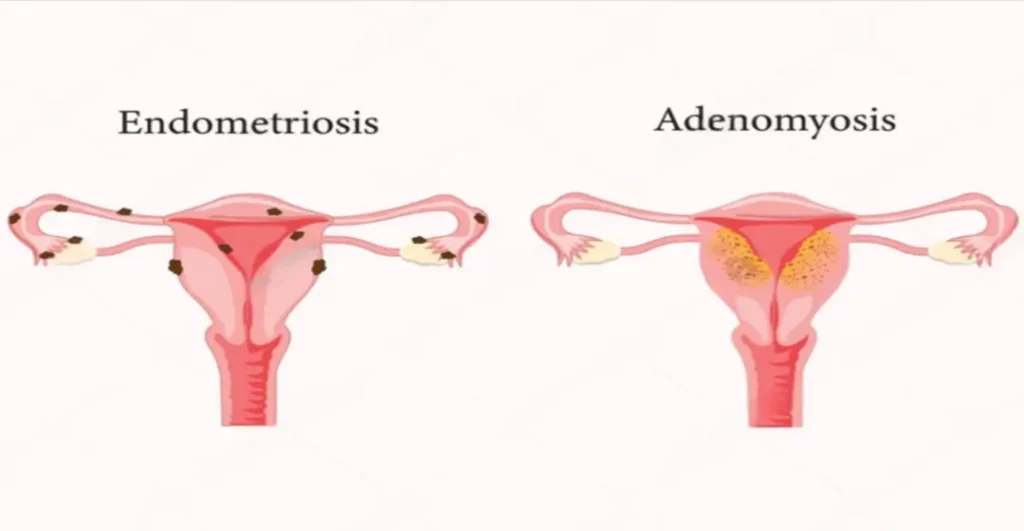
- Untreated Endometriosis & Adenomyosis:
These inflammatory conditions are highly prevalent in Indian patients and often underdiagnosed.
-
Endometriosis: Endometrial-like tissue grows outside the uterus.
-
Adenomyosis: Endometrial tissue infiltrates the uterine muscle.
Both conditions create a pro-inflammatory pelvic environment that disrupts embryo–endometrium crosstalk and reduces implantation potential.
- Multiple or Cavity-Distorting Uterine Fibroids:
Non-cancerous growths that can distort the uterine cavity or impair blood flow to the lining, physically preventing the embryo from nesting.
Submucosal or large intramural fibroids are particularly associated with implantation failure.
- Chronic Endometritis:
A persistent, low-grade inflammation of the endometrial lining, often caused by subtle infections. This is a microscopic factor that cannot be seen on a standard ultrasound.
Chronic endometritis is one of the most commonly missed causes of RIF in India.
- Immunological Factors:
Situations where the mother’s immune system fails to recognize and "accept" the embryo, instead treating it as a foreign threat.
Don't let chronic endometritis or silent TB ruin your next transfer. Get a specialized biopsy and hysteroscopic review to ensure your lining is truly healthy.
If Your Case Was Labeled “Idiopathic,” What Does That Mean?
“Idiopathic” does not mean untreatable. It simply means that the cause was not visible using standard diagnostic tools.
Patient Tip: If your RIF was called idiopathic, confirm that you were screened for chronic endometritis using CD138 or MUM-1 staining. Microscopic inflammation is frequently missed in routine IVF centers.
This is why Dr. Jay Mehta emphasizes the need for a "deep dive" using advanced technical audits.
By moving beyond basic scans to endometrial immune profiling or diagnostic hysteroscopy, we often find that an "idiopathic" case actually has a hidden, treatable microscopic cause.
Addressing these common causes requires more than just a new stimulation protocol; it requires surgical and technical precision.
At our RIF clinic in Mumbai, we specialize in correcting these pathologies—such as performing advanced laparoscopic surgery for endometriosis or specialized treatments for a thin endometrium—before the next embryo transfer.
Can Good or Euploid Embryos Still Fail to Implant?
Yes, good-quality or euploid (chromosomally normal) embryos can and do fail to implant
Even when a "Top Quality Embryo" (TQE) is transferred—and even more surprisingly, even when that embryo is a genetically tested, chromosomally normal euploid embryo—implantation can still fail.
In clinical practice, this is one of the most difficult scenarios for both the patient and the clinician.
When the "perfect" seed is planted in seemingly "perfect" soil and fails to grow, it points toward the deepest mysteries of reproductive science.
Chromosomal normality is essential—but it is not the entire implantation story.
The Hidden Science: Why "Genetically Normal" Isn't Always Enough?
A euploid embryo has the correct number of chromosomes (46, XX or 46, XY), but chromosomal count is only one part of the success equation.
Modern research is currently diving into three advanced "Omics" to find out why these embryos sometimes fail:
- Transcriptomics: Genes must not only be present—they must activate at the correct time.
Implantation requires precise gene expression during a narrow window. If key implantation genes fail to “switch on” at the right microsecond, the embryo-endometrium dialogue may fail.
- Proteomics: This is the study of proteins. For a successful pregnancy, both the embryo and the uterine lining (endometrium) must secrete specific proteins to communicate with each other.
- Metabolomics: This focuses on embryo metabolism. It studies the chemical signatures and energy usage of the embryo to identify "embryo exhaustion," which might not be visible under a microscope.
While these are currently researched in clinical settings and are not yet routine in India, they represent the future of how we will solve "unexplained" failure.
Controlling the "Controllables" in Embryo Transfer
When a good embryo fails, Dr. Jay Mehta emphasizes that we must first audit the clinical steps to ensure they were performed flawlessly. At our clinic, we focus on:
- Expert Transfer Technique: Every embryo transfer must be performed by a highly skilled specialist, preferably under continuous ultrasound guidance, to ensure the embryo is placed at the exact "sweet spot" of the fundus.
- Advanced Lab Protocols: We assume the freezing and thawing (cryopreservation) techniques were perfect. A technically upgraded lab ensures that the embryo's vitality is not compromised during these transitions.
- Precision Endometrial Preparation: The lining must be prepared using a protocol tailored specifically to the patient’s hormonal profile, ensuring the "window of implantation" is wide open.
Patient Tip: Ask your clinic if they use time-lapse imaging or spindle assays. These tools provide more data on embryo health and metabolism than standard visual grading, helping us understand why a "good" embryo might have hidden weaknesses.
Maintaining Confidence Through Realistic Expectations
One of the greatest risks in RIF is the loss of patient confidence.
If a clinician does not provide a realistic, transparent picture of why a transfer might fail, the patient may feel the system has failed them and abandon their journey entirely.
Dr. Jay Mehta’s philosophy is built on candor and empathy. By explaining that science is still an evolving enigma, we help patients understand that a failure isn't necessarily their "fault" or a sign that they will never conceive.
It simply means we need to look closer at the technical "fine points."
If your "perfect" embryos are failing, it’s time to look at the advanced factors routine clinics miss. Consult with India’s leading RIF specialist, Dr. Jay Mehta, to discuss your next scientific steps
When Is PGT-A Strongly Recommended After Failed IVF Transfers?
If a patient has experienced one or two failed embryo transfers—especially with good-quality embryos—Pre-implantation Genetic Testing for Aneuploidies (PGT-A) becomes strongly recommended.
At this stage, continuing blind transfers becomes trial-and-error medicine.
PGT-A helps determine whether the embryo itself is the cause of failure—or whether attention must shift toward the uterus or immunological factors.
The Role of PGT-A in Recurrent Implantation Failure
Pre-implantation Genetic Testing for Aneuploidies (PGT-A) is a critical tool in solving the puzzle of Recurrent Implantation Failure (RIF).
It allows us to look beyond the visual "grade" of an embryo and determine its chromosomal health.
In many cases of RIF, the reason for failure is not the uterus but a "hidden" genetic abnormality in an embryo that otherwise looks perfect under the microscope.
1. How is PGT-A performed?
The procedure is a high-precision microscopic surgery performed on a Day 5 embryo (blastocyst):
- The Biopsy: A specialist embryologist extracts approximately 3 to 5 cells from the trophectoderm, which is the outer layer of the embryo that eventually forms the placenta. The inner cell mass (which becomes the baby) remains untouched.
- DNA Analysis: These cells are cultured to extract and amplify their DNA. We then study the chromosomal architecture to ensure the embryo has the correct number of chromosomes (46).
- The Goal: To identify euploid (chromosomally normal) embryos, which have the highest probability of successful implantation and a healthy pregnancy.
2. Non-Invasive Alternatives (NICS)
Non-Invasive Chromosomal Screening (NICS) is an emerging alternative.
Instead of taking a physical biopsy, this technique tests the fluid surrounding the embryo in the culture dish, where the embryo naturally sheds its genetic material.
While this sounds ideal, Dr. Jay Mehta warns that it requires extremely strict culture conditions.
Most fertility clinics in India are not yet optimized for this level of precision. At our center in Mumbai, we strongly evaluate the laboratory's readiness before recommending non-invasive testing to ensure accuracy.
3. Can Previously Frozen Embryos Still Be Tested?
This is a common concern for patients who have already cryopreserved embryos at other clinics and are seeking a second opinion after a failure.
The answer is yes. It is entirely safe to:
- Unfreeze (thaw) the embryo.
- Perform the biopsy for PGT-A.
- Refreeze the embryo.
The technical secret lies in the timing: as long as the entire process is completed in less than 54 minutes, the embryo's vitality is preserved.
This requires a highly trained embryology unit with the technical expertise to handle "thaw-biopsy-refreeze" cycles—a service we routinely provide for patients seeking an answer to their previous failures.
4. Why Does Expertise Matter So Much?
PGT-A is not a routine lab task—it is microsurgery at the cellular level.
Performing PGT-A is technically challenging. If done incorrectly, it can cause permanent and irreversible damage to the embryo.
In India, many patients seek a second opinion from us because their original clinic lacked the facility or the expert embryologist to perform this biopsy safely.
This is why Dr. Jay Mehta emphasizes that the procedure must be carried out meticulously under strict aseptic precautions by a specialist with a high volume of experience.
When Should You Seriously Consider PGT-A?
PGT-A is strongly recommended if:
- You have had 1–2 failed high-grade embryo transfers
- You are above 35 years of age
- You have experienced recurrent miscarriages
- You have limited embryos and want to optimize selection
- You want to reduce repeated emotional and financial loss
Does Embryo Morphology Really Predict Implantation Success?
Embryo morphology—the way an embryo "looks" under a microscope—is a primary tool used by embryologists to predict success.
However, morphology is a strong indicator; it is not a perfect predictor.
Even “Grade A” embryos can fail. And sometimes average-looking embryos succeed.
At a specialized RIF clinic, we have moved beyond simple visual inspection to use artificial intelligence and time-lapse technology to select the best possible embryo.
1. Traditional Embryos Grading: The Visual Standard
Traditionally, embryologists manually grade embryos (specifically Day 5 blastocysts) based on two main components:
- Inner Cell Mass (ICM): The portion that develops into the baby.
- Trophectoderm (TE): The outer layer that forms the placenta
These are assigned scores (like AA, AB, or BB). While this standard classification is still used by most units in India, it is subjective and depends on the individual embryologist's eye.
2. AI and Time-Lapse Imaging: The Modern Standard
In advanced RIF clinics, manual grading is being replaced by AI-based algorithms integrated with time-lapse incubators.
- Continuous Monitoring: Time-lapse incubators take images every 10–20 minutes, creating a developmental video of the embryo from fertilization to the blastocyst stage.
The embryo remains undisturbed inside the incubator, maintaining stable conditions.
- AI-Based Analysis: The AI checks specific developmental milestones (checkpoints) that the human eye might miss, guiding the clinician toward the embryo with the highest biological potential.
AI doesn’t replace the embryologist—it augments decision-making with objective data.
- Non-Invasive: Because the embryo is never removed from the incubator for checking, its environment remains perfectly stable.
3. The "Beauty vs. Genetics" Paradox
It is vital to understand that an embryo's "looks" can be deceiving:
- The "Beautiful" Failure: Some embryos look morphologically "perfect" but fail to implant because they are chromosomally abnormal (aneuploid).
- The "Average" Success: Some embryos that look average or "less than perfect" turn out to be genetically normal (euploid) and result in a healthy pregnancy.
This paradox is why we strongly encourage PGT-A (genetic testing). Morphology tells us about the embryo's current growth, but genetics tells us about its future potential.
4. Understanding the 45-50% Success Threshold
Even with a "top quality" Day 5 embryo selected through the best morphological standards, the implantation potential typically peaks at 45–50%.
Because current science cannot yet "see" every molecular variable (like metabolomics or proteomics), we cannot offer a 100% guarantee.
5. Does Combining AI and PGT-A Improve Outcomes?
For patients with previous IVF failures, combining:
- AI-based morphokinetic analysis
- Time-lapse imaging
- PGT-A (genetic testing for aneuploidy)
can significantly improve embryo selection accuracy and reduce “trial-and-error” transfers.
This approach does not guarantee pregnancy, but it improves precision and shortens the time to pregnancy in appropriately selected patients.
Expert Insight: Morphology is a great starting point, but for patients with previous failures, we must look deeper. Combining AI grading with genetic testing is the only way to break past the standard 50% success ceiling.
If you have failed multiple cycles with "good-looking" embryos, it is time to look deeper.
Our laboratory in Mumbai specializes in using AI and time-lapse technology to find the technical reasons for your previous failures.
Are you frustrated by repeated failures despite having "Grade A" embryos? You can request an Embryo Video Audit with Dr. Jay Mehta to see how AI-based time-lapse monitoring could have identified hidden developmental hurdles in your previous cycles.
Would you like me to help you interpret the grading (e.g., 3BB, 4AA) of your previously transferred embryos to see if they fit the criteria for further genetic investigation?
AI-Based Embryo Selection: A Game-Changer for IVF Success . This video explains how AI-based selection and time-lapse imaging provide a more precise way to track embryo development, offering new hope for those with previous IVF failures.
Can Mosaic Embryos Be a Solution in Recurrent Implantation Failure (RIF)?
A mosaic embryo is a unique genetic finding where an embryo contains two or more populations of cells with different chromosomal makeup—some cells are normal (Euploid), while others are abnormal (Aneuploid).
In the context of Recurrent Implantation Failure (RIF), mosaic embryos sit in a "gray area."
They are neither perfectly normal nor completely abnormal, presenting a complex choice for couples who may not have any fully normal embryos available.
How Is Mosaicism Classified?
When genetic testing (PGT-A) identifies mosaicism, we categorize the embryo based on the percentage of abnormal cells found in the biopsy:
- Low-Level Mosaic (30%–50%): These embryos have a higher proportion of normal cells and generally have better implantation potential and lower miscarriage rates.
- High-Level Mosaic (50%–70%): These embryos have a majority of abnormal cells. While they can still lead to a healthy pregnancy, the risks of failure or miscarriage are significantly higher.
Key Scientific Fact: If an embryo has less than 20% abnormal cells, it is clinically classified as Euploid (normal). If it has more than 80%, it is classified as Aneuploid (abnormal).
The Phenomenon of "Auto-Correction"
One of the most fascinating aspects of mosaic embryos is their ability to undergo auto-correction. As the embryo develops and implants, it can sometimes "self-correct" by:
- Selective Proliferation: Normal cells divide faster than abnormal ones.
- Apoptosis: The embryo naturally identifies and eliminates the abnormal cells.
- Confined Placental Mosaicism: Pushing the abnormal cells into the trophectoderm (which becomes the placenta) while keeping the inner cell mass (which becomes the baby) genetically normal.
Because of this "Shepherd Mechanism," mosaic embryos have resulted in thousands of healthy live births worldwide.
The Risks Involved
While success is possible, an RIF specialist must provide a transparent picture of the risks. If the genetic rearrangement (auto-correction) does not occur:
- Lower Implantation Rates: Compared to fully euploid embryos, mosaic embryos are less likely to "stick."
- Higher Miscarriage Risk: If the genetic rearrangement or auto-correction does not occur successfully, the pregnancy may result in a first-trimester abortion.
- Uncertainty: While rare, there is a theoretical risk of the child having a chromosomal syndrome, though most successful mosaic pregnancies result in chromosomally normal babies.
In India, there are currently no strict legal guidelines prohibiting the transfer of mosaic embryos.
At our clinic, we believe in patient autonomy. We provide "crystal clear" instructions and genetic counseling, allowing the couple to make an informed decision based on their specific journey and the number of embryos they have left.
| Embryo Type | Implantation Potential | Miscarriage Risk | Priority |
|---|---|---|---|
| Euploid | High (~60-70%) | Low | 1st Priority |
| Low-Level Mosaic | Moderate (~35-45%) | Moderate | 2nd Priority |
| High-Level Mosaic | Lower (~20-30%) | Higher | 3rd Priority |
| Aneuploid | Near Zero | Very High | Not Recommended |
Rates vary depending on maternal age, uterine factors, and specific chromosomal involvement.
Does the Type of Mosaicism Matter?
Yes—significantly.
Outcomes differ depending on:
-
Segmental mosaicism (partial chromosome involvement)
-
Whole chromosome mosaicism
-
Specific chromosome affected (e.g., some chromosomes are more compatible with live birth than others)
A detailed interpretation of the PGT-A report is crucial before making a transfer decision.
When Might Mosaic Transfer Be Considered?
Mosaic embryo transfer may be reasonable when:
-
No euploid embryos are available
-
Additional IVF cycles are not feasible
-
The couple understands the risks
-
Proper genetic counseling is completed
-
Invasive prenatal testing (CVS or amniocentesis) is planned if pregnancy occurs
The Key Takeaway for RIF Patients
Mosaic embryos are not “failed embryos.” They are embryos with uncertain but real potential.
In recurrent implantation failure cases, especially when no euploid embryos remain, they may offer another scientifically reasonable chance—provided the decision is informed, individualized, and guided by updated international data.
If you would like, you can share:
-
The percentage of mosaicism
-
Whether it is a segmental or whole chromosome
-
The chromosome involved
I can help you understand the general risk profile and what current data suggests about outcomes.
In complex fertility decisions, clarity reduces fear—and informed choice restores control.
Can the Uterus Cause Recurrent Implantation Failure?
Yes, the uterus is a primary factor in recurrent implantation failure.
While much of the focus in IVF is often placed on the embryo, the success of a pregnancy is heavily dependent on the entire uterus—including its muscular health, its size, and any underlying pathology.
For an embryo to implant successfully, we must ensure that the uterine environment is absolutely normal.
The "Soil" Matters as Much as the "Seed"
In fertility care, we often compare the embryo to a seed and the uterus to the soil.
Even the healthiest "seed" cannot grow if the "soil" is not receptive.
At Shree IVF Clinic, we find that an altered uterus often leads to an altered endometrium (the inner lining), which significantly diminishes the implantation potential of the embryo.
There are three critical ways the uterus influences your success:
- Abnormal Uterine Contractions: The muscular wall of the uterus is not static; it has natural movements. However, if you have conditions like Endometriosis, Fibroids, or Adenomyosis, these contractions can become irregular or hyperactive. This "hostility" can physically prevent an embryo from settling into the lining.
- Structural and Muscular Issues: The overall size and the muscular integrity of the uterus play a vital role. Pathology within the uterine wall doesn't just sit there; it changes the biological environment of the entire organ.
- The Silent Impact of Tuberculosis: Specifically in India, we must be very cautious of Genital Tuberculosis. It often progresses silently, causing permanent damage to the endometrium and effectively destroying its ability to support an embryo.
Why Is Precision Diagnosis Essential?
This is exactly why we insist on a "decisive ultrasound" and a deep-dive study of the inner lining for every patient who comes to us with a history of failed IVF cycles. We need to see the full picture before moving forward.
One of the challenges in modern fertility care in India is that many clinics bypass these uterine issues.
Correcting pelvic pathology requires high-level technical expertise and a well-equipped operating theatre for advanced laparoscopic or robotic surgeries.
Because not all centers have these facilities, patients are often guided toward IVF while severe pelvic issues remain unaddressed.
Restoration Before Intervention
The most encouraging fact I share with my patients is this: once we correct the underlying pelvic pathology—such as removing a fibroid or treating endometriosis—the results are transformative.
In fact, more than 60% of patients who have these issues corrected through expert surgery end up conceiving naturally within the following year, without needing IVF at all.
If you have faced the heartbreak of a failed cycle, it is time to look closer at the uterine factor.
Our goal at Shree IVF Clinic is to provide the clinical clarity you need to stop the cycle of failure.
We focus on healing the uterus first to ensure that when we do transfer an embryo, it has the best possible home to grow in.
Whether you are seeking a second opinion or a comprehensive evaluation of your uterine health, we are here to provide evidence-based, empathetic guidance.
Does Endometrial Receptivity Really Matter in Recurrent Implantation Failure (RIF)?
Endometrial receptivity is the critical "window of time" when the uterine lining is ready to accept an embryo.
However, the science of testing this window is still evolving, and most modern data suggests that routine commercial tests—like the ERA—rarely offer a significant clinical benefit for the average patient.
While the lining's receptivity is vital for a healthy embryo (Euploid) to attach, we must be cautious about expensive tests that may not actually increase your chances of having a baby.
Is the ERA Test Worth the Investment for My IVF Journey?
For years, the Endometrial Receptivity Array (ERA) was widely promoted, primarily based on European data, as a way to find the perfect timing for embryo transfer.
However, at Shree IVF Clinic, we prioritize evidence-based medicine over trends.
We have largely stopped performing the ERA test since 2023. Why? Because global clinical outcomes have shown that it doesn't offer a significant advantage for most patients.
It often adds a heavy financial burden—approximately ₹40,000 to ₹50,000 in India—without a clear medical return.
Furthermore, the results are only valid for the very next cycle and require specific hormone (HRT) preparations, making it a very rigid and costly path.
Expert Tip: If you are self-financing your IVF journey, always ask your consultant: "Will this test statistically improve my live birth rate, or is it just an added cost?" Transparency is the first step to a successful pregnancy.
When Should I Actually Consider Endometrial Testing?
While we move away from routine testing, there are very specific, rare clinical situations where a receptivity test might still be helpful.
- Severe Obesity: Patients with a very high BMI may have a shifted window of implantation.
- Extreme PCOS: Cases of Polycystic Ovary Syndrome that do not respond to standard protocols.
Apart from these exceptions, many reputed fertility clinics worldwide and government-led health organizations have moved away from this test because it simply doesn't add enough clinical value to justify the cost.
Need a Second Opinion? If you have been advised to take an ERA test just because you have frozen embryos left, I recommend a formal consultation to see if your embryos should be genetically tested instead.
Why Am I Facing Recurrent Implantation Failure (RIF)?
If you have experienced multiple failed cycles, it is natural to want to test everything. However, the "seed" (the embryo) is often more important than the "timing" of the soil.
| Feature | Endometrial Receptivity (ERA) | Embryo Genetic Testing (PGT-A) |
|---|---|---|
| Primary Goal | Finds the "timing" of the lining | Checks if the embryo is "Euploid" (healthy) |
| Success Factor | Debated; low impact for most | High, healthy embryos are the #1 success factor |
| Cost in India | ₹40,000 - ₹50,000 | Varies by number of embryos |
| Our Recommendation | Generally avoided since 2023 | Highly recommended for recurrent failure |
Clinical Guidance: If you have frozen embryos at a clinic and have faced failure, a more viable option is often to undergo genetic testing (PGT-A) on those embryos if you haven't already.
What Are the Best Next Steps for Couples in Mumbai?
In a country like India, we also have to look for "silent" factors that tests like the ERA might miss, such as genital tuberculosis, which can permanently damage the lining.
My Recommendations for You:
- Seek a Second Reference: Before committing to high-cost tests, speak with a reproductive immunologist or a specialized fertility consultant.
- Focus on Embryo Integrity: Ensure you are transferring a chromosomally normal embryo before blaming the "window" of the lining.
- Comprehensive Uterine Evaluation: A decisive ultrasound by an expert can often find structural issues that a biopsy might miss.
Take the Next Step with Confidence:
As an expert in advanced laparoscopy and reproductive medicine in Mumbai, I focus on finding the root cause of failure rather than suggesting unnecessary "add-on" treatments.
Let's look at your previous cycles together to build a path that is both scientifically sound and ethically responsible. Contact Shree IVF Clinic Mumbai to evaluate your uterine health with Dr. Jay Mehta
Has My Window of Implantation Shifted—And Is That Why My IVF Failed?
Yes—a displaced window of implantation can absolutely cause recurrent implantation failure.
If the uterine lining becomes receptive too early or too late, even a high-quality or genetically normal (euploid) embryo will fail to attach.
In a natural cycle, this window is roughly 24 hours, but for patients on a medicated HRT protocol, it can shrink to a narrow 6 to 8 hours. That means timing must be extremely precise.
If the embryo and uterus are not synchronized, implantation will not occur—even when everything else appears “perfect.”
Why Does the "Timing" of My Uterus Get Displaced?
A displaced window means your uterus is opening its "doors" either too early or too late for the embryo transfer. This lack of synchronization is rarely random.
At Shree IVF Clinic, we find that this shift is usually driven by specific biological "noise" in the pelvis:
- Pelvic & Uterine Pathology: Conditions like endometriosis or acute pelvic inflammation create an inflammatory environment that disrupts natural hormonal signaling.
Managing endometriosis through proper treatment—and sometimes lifestyle measures such as an endometriosis diet—can help reduce inflammation and support better uterine function.
- Chronic Inflammation: Hidden infections in the uterine lining (chronic endometritis) are incredibly common causes of a shifted window.
- Lifestyle & Hormones: Factors such as extreme obesity or specific hormonal deficiencies can alter how the uterus responds to progesterone, causing the timing to drift.
In some women, underlying pelvic conditions such as severe endometriosis may also require surgical treatment to restore a healthy uterine environment. At our center, we focus on advanced yet low-cost endometriosis surgery designed to remove the disease effectively while preserving fertility.
Next Step: If you have endometriosis or a history of pelvic pain, your window might be affected. Call 1800-268-4000 to schedule a specialized pelvic evaluation with our team
How Can We Correct a Shifted Implantation Window?
If you have experienced recurrent failure, repeating the same protocol is not the solution. We focus on "resetting" the uterine environment so the window returns to its natural, predictable state.
1. Diagnostic Hysteroscopy: We perform a detailed look inside the uterus to rule out chronic pathology. This allows us to see inflammation or micropolyps that a standard ultrasound might miss.
2. The 21-Day Healing Course: If inflammation is detected, we treat it with a specific 21-day course of antibiotics to clear the "hostile" environment.
3. Restoring the Microbiome: Following antibiotics, we prescribe oral probiotics for three months. This restores the healthy bacterial balance (Lactobacillus), which is essential for a stable implantation window.
4. Precise Drug Calibration: Once the environment is healthy, we precisely calculate your medication timing to ensure the embryo meets the lining at its peak.
Take Action: Concerned about hidden inflammation? Book a diagnostic hysteroscopy consultation in Mumbai to check your uterine health.
What Success Rates Can Be Expected After Correction?
When we synchronize a chromosomally tested (euploid) embryo with a corrected, perfectly timed window, the clinical pregnancy rate is approximately 45% to 50%.
This is a massive leap in success for couples who have previously faced failure. It highlights that the "correct calculation" of drugs and the "health of the cavity" are just as important as the embryo itself.
Dr. Jay Mehta’s Advice: Precision always beats repetition. In my practice, we don't move forward with a transfer until we are certain the 'soil' is quiet and the timing is calibrated to the hour. This is how we turn recurrent failure into a successful pregnancy.
What Should You Do Before Your Next Transfer?
If you are planning your next steps after a previous failure, here is the protocol I recommend:
- Investigate the "Silent" Barrier: Ask for a hysteroscopy to check for chronic endometritis before your next cycle.
- The Probiotic Prep: Give your body 3 months to optimize its uterine microbiome if you have a history of inflammation.
- Calibrate to the Hour: Ensure your clinic is timing your progesterone start time precisely, especially in HRT cycles where the window is very narrow.
As a specialist in fertility and complex uterine health in India, I focus on the intricate details of the uterine environment that others might overlook.
We don't just "do IVF"; we engineer a successful environment. If you feel your timing has been a factor in your previous failures, let’s build a protocol tailored to your specific biology.
Contact Dr. Jay Mehta at Shree IVF Clinic for a second opinion on your recurrent implantation failure.
Thin Endometrium and Recurrent Implantation Failure: What Truly Matters?
A thin endometrium does not automatically mean you cannot conceive—but it does demand clarity, precision, and realism.
A thin endometrium—defined as a lining that refuses to grow beyond 5 mm despite medical intervention—is one of the most challenging obstacles in fertility.
While we typically strive for a lining of 7–8 mm, it is important to know that achieving a pregnancy with a thin endometrium is possible.
However, thickness alone does not determine success
Tissue health, vascularity, inflammation status, and structural integrity are often more important than the number on the ultrasound screen.
Why Does the Endometrium Remain Thin?
At Shree IVF Clinic, we treat the endometrium with the clinical respect it deserves.
In many cases, we encounter "idiopathic" thin endometrium, meaning there is no clear, identifiable cause despite exhaustive testing.
However, in the Indian context, specific factors often play a leading role:
- Silent Endometrial Tuberculosis: This is the most common cause of persistent lining damage in India. It can silently scar the tissue, permanently affecting its growth potential before you even notice a symptom.
- Asherman’s Syndrome (Intrauterine Adhesions): Previous procedures like D&C (Dilatation and Curettage) can cause adhesions or scarring inside the cavity. This is notoriously difficult to treat; even with repeated surgeries, the success rate for implantation remains low.
- Adenomyosis: Conditions affecting the uterine muscle can distort the "junction" between the muscle and the lining, making it nearly impossible for the endometrium to thicken naturally.
Take Action: If you have a history of pelvic infections or multiple D&C procedures, your lining health needs a closer look. Schedule a decisive 3D ultrasound at Shree IVF Clinic to evaluate your lining.
Evaluating Common Treatments and Their Reality
The medical world is full of "miracle cures" for a thin lining. At our clinic, we believe in providing honest, science-backed guidance rather than promising the moon.
- PRP (Platelet-Rich Plasma) and G-CSF: While intrauterine injections (like PRP) are popular in India, their success is not guaranteed. We use these therapies with caution and only when clinically indicated.
- Stem Cell Therapy: We have explored autologous bone marrow stem cell therapy. While it is an advanced option, our experience shows it benefits patients in only about 55% to 60% of situations.
- Medications: Literature consistently questions the roles of Sildenafil (Viagra), high-dose Estradiol, or G-CSF. These should be used with a strong amount of caution, as they rarely provide a breakthrough for fundamentally damaged tissue.
Dr. Jay Mehta’s Advice: Honest counseling sometimes encourages patients to seek out doctors who promise impossible results.
However, many eventually return to us because we tell the absolute truth: if the lining is chronically thin but the environment is 'quiet' and healthy, implantation can still happen. We focus on tissue quality over millimeter count.
Pregnancy Risks with Thin Endometrium
A persistent thin endometrium isn't just an IVF challenge; it carries risks throughout a pregnancy. Women with a thin lining who do conceive must be monitored closely for:
- Recurrent miscarriages.
- Preterm deliveries.
For a subset of women where the lining is permanently destroyed, we must have a realistic conversation.
If the endometrium refuses to respond to all therapies, alternative options like surrogacy may eventually be the most viable path to a healthy baby.
Expert Insight: Understanding the long-term risks is essential for a safe pregnancy. Speak with our fertility specialists in Mumbai to discuss your personal prognosis and pregnancy safety.
If you are struggling with a lining that won't grow, here is how we can move forward:
- Rule Out the "Silent" Killers: Ensure you have been thoroughly screened for genital TB and adenomyosis before attempting more transfers.
- Avoid Surgical Trauma: If you have Asherman's Syndrome, avoid repeated, aggressive hysteroscopic surgeries, which can cause more harm than good to delicate tissue.
- Look Beyond the Thickness: If the causes are idiopathic (unknown), it is often easier to achieve implantation than in cases caused by scarring.
Expert Perspective: As a specialist in managing recurrent implantation failure, I understand the frustration of a thin lining.
My goal is to give you a realistic picture of your uterine health and build a strategy based on what the science actually supports.
Are you tired of "miracle" treatments that don't manifest? Let’s conduct an honest evaluation of your line's true potential.
Could Chronic Endometritis Be the Silent Reason Behind My Recurrent Implantation Failure?
Yes—chronic endometritis is one of the most common and most overlooked causes of recurrent implantation failure (RIF).
Chronic endometritis is a persistent, low-grade inflammation of the uterine lining that often stays "silent" because it rarely causes symptoms.
The good news is that once correctly diagnosed, it is one of the most treatable and satisfying conditions to resolve in fertility care.
What Exactly Is Chronic Endometritis?
Chronic endometritis is not an acute infection. It is a subtle, smoldering inflammatory state of the endometrium.
Instead of dramatic symptoms, it causes:
-
Microscopic immune activation
-
Poor endometrial maturation
-
Disrupted implantation signaling
-
Altered uterine microbiome
An embryo may reach the uterus perfectly, but the lining is not biologically welcoming.
Why Is Chronic Endometritis So Hard to Detect?
Unlike acute infections that cause pain or fever, chronic endometritis is "irritating" to treat because it is nearly invisible during a routine check-up.
Most patients have no typical symptoms at all. At Shree IVF Clinic, we identify this condition through specialized diagnostic tools:
- Hysteroscopy: We look for specific "strawberry-colored patches" along the endometrial wall, which are tell-tale signs of inflammation.
- Hysteroscopic Guided Biopsy: We take a tiny sample of the lining for histopathological and microbiological testing to confirm the diagnosis before starting antibiotics.
- Advanced Markers (MUM-1): In the past, doctors used CD138 to find plasma cells. Today, we use MUM-1, a far more specific marker that helps us identify microscopic chronic endometritis with much higher accuracy.
Dr. Jay Mehta’s Tip: If your endometrium stays persistently thin or looks "hazy" very early in your cycle when exposed to estrogen, it could be an early sign of chronic endometritis. Don't ignore these subtle ultrasound cues.
Our Proven "Reset and Restore" Treatment Protocol
Once correctly diagnosed, the treatment is smooth and straightforward. More than 90% of our patients experience a significant benefit in their fertility outcomes after following our protocol:
1. The 21-Day Antibiotic Course: A targeted 21-day course to eliminate the underlying infection.
2. The 90-Day Probiotic Phase: Following antibiotics, we use oral probiotics for three months to completely restore the endometrial microbiome.
Usually, once the antibiotic phase is complete, a repeat biopsy is not warranted. This comprehensive approach helps in both the healthy development of the endometrium and the overall success of the implantation.
Take Action: Have you had multiple failed transfers with no clear explanation? A simple 21-day treatment might be the missing link. Consult with our experts about our Endometrial Reset Protocol
Beyond Infection: The Role of uNK Cells and Spiral Arteries
Beyond clearing infection, successful implantation requires perfect coordination between the embryo and the uterus. This is where uNK cells (Uterine Natural Killer cells) play a vital role.
- Coordination: uNK cells act as "communicators" between the embryo and the lining.
- Blood Supply: They are essential for the development of spiral arteries, which ensure enough blood reaches the embryo to allow the pregnancy to continue successfully.
We often test the concentration of these cells because they must be present at specific levels for the pregnancy to be sustainable.
Clinical Insight: Testing for uNK cells along with MUM-1 gives us a complete map of your uterine health, moving beyond just "looking" at the lining to understanding how it functions.
Practical Next Steps for Your Journey
If you are navigating the frustration of RIF in Mumbai, focusing on the microscopic health of your uterus is essential:
- Demand Specificity: Ensure your clinic uses MUM-1 markers for plasma cell isolation rather than the older CD138 method.
- Restore the Microbiome: Don't skip the probiotic phase; a healthy bacterial balance is just as important as clearing the infection.
- Focus on Satisfaction: Remember that this is one of the most rewarding conditions to treat—the transition from a "hostile" to a "healthy" uterus happens relatively quickly.
As a specialist in resolving complex cases of recurrent implantation failure, I focus on the microscopic details that others might miss. We don't just treat the infection; we engineer a receptive home for your future child.
Are you ready to clear the silent barriers to your pregnancy? Let’s do a thorough evaluation of your uterine health to help ensure your next transfer is successful. Consult with Dr. Jay Mehta at Shree IVF Clinic for a Truthful Evaluation of Your Endometrium
Should Adenomyosis Be Surgically Corrected Before Attempting IVF for Recurrent Implantation Failure?
Yes—in properly selected patients, correcting adenomyosis or deep endometriosis first can significantly improve implantation rates and may even restore natural fertility.
Adenomyosis and endometriosis are leading causes of recurrent implantation failure (RIF) because they create a hostile, inflammatory environment within the uterine muscle and the pelvis.
While many clinics suggest rushing into IVF despite these conditions, the clinical truth is that successful implantation is significantly higher—and often occurs naturally—only after these pathologies are surgically corrected by a specialist.
The Reality of Treating Adenomyosis in India
In India, many fertility specialists hesitate to refer patients to "Centers of Excellence" for endometriosis due to concerns about losing the patient.
Consequently, patients are often pushed into IVF cycles while still suffering from deep endometriosis or adenomyosis.
This approach is often counterproductive. Attempting egg retrieval or embryo transfer in a patient with Grade 4 endometriosis or a distorted, adenomyotic uterus is extremely difficult and rarely leads to a successful pregnancy.
At Shree IVF Clinic, we believe in a "surgery first" approach for a reason: the data support it.
- Expert Success Rates: If you undergo surgery with an endometriosis specialist like us, the chance of the disease returning is less than 5%.
- Natural Conception: Most surprisingly, more than 60% of our patients conceive naturally within the first year after surgery, without ever needing in vitro fertilization treatment.
Pro Tip: Don't let a clinic rush you into an IVF cycle if you have unaddressed adenomyosis. Correcting the "home" first is the most ethical and successful path to parenthood. Consult with Dr. Jay Mehta for a specialized Endometriosis & adenomyosis treatment in Mumbai, India
Advanced Surgical Techniques Used in Adenomyosis: Restoring Uterine Health
Treating adenomyosis requires specialized technical skills that go beyond standard laparoscopy.
We utilize advanced techniques to restore the uterus to its normal function:
1. Flap Surgery (Osada Procedure): A reconstructive technique to remove the adenomyotic tissue while rebuilding a strong uterine wall. This improves uterine function and reduces abnormal contractions.
2. Microwave Ablation: A modern, minimally invasive method to treat adenomyosis, especially when it involves the lateral walls of the uterus.
3. Combination Therapy: Often, we use both methods, excision and ablation, to ensure the uterus is thoroughly cleared of disease.
The Recovery Period: After surgery, we typically advise patients to wait 4 to 6 months before attempting an embryo transfer. This allows the uterus to heal and become the stable environment an embryo needs.
Debunking the Myth: Does Surgery Weaken the Uterus?
A common fear among patients is that surgery for endometriosis or adenomyosis will weaken the uterus for future pregnancy. This is incorrect information.
When performed by a super-specialist, these surgeries actually strengthen your reproductive potential. To give you perspective:
- We perform more than 2,000 surgeries for endometriosis and adenomyosis every year across India.
- Following successful surgery, we see implantation rates increase by as much as 20%.
Expert Insight: The confidence in these results comes from years of high-volume, specialized experience. Surgery, when done right, is a restorative process, not a destructive one. Speak with our surgical team in Mumbai about your concerns.
Practical Next Steps If You Have Adenomyosis or Grade 4 Endometriosis
If you are facing recurrent failure and have been diagnosed with Adenomyosis or Endometriosis, here is how to protect your journey:
- Demand a Specialist: Ensure your surgeon specializes in Deep Endometriosis and Adenomyosis specifically, rather than general gynecology.
- Be Patient with Healing: Respect the 4–6 month healing window after surgery; it is the secret to a high implantation rate.
When Is IVF Still Necessary?
Surgery does not eliminate the need for IVF in every case. Women with reduced ovarian reserve, advanced maternal age, and male factor infertility may still require assisted reproduction.
However, correcting the uterine and pelvic environment first can dramatically improve outcomes.
As a referral unit for advanced endometriosis for patients across India, my goal is to stop the cycle of failed IVF.
We focus on specialized surgical correction to give you the best chance of a natural pregnancy or a successful IVF outcome.
Are you ready to address the root cause of your implantation failure?
Let’s evaluate your uterine health and discuss a surgical plan that puts your long-term success first.
Why Is Hysteroscopy Considered the Gold Standard for Diagnosing Recurrent Implantation Failure (RIF)?
Hysteroscopy is perhaps the most critical diagnostic tool for any patient facing Recurrent Implantation Failure (RIF).
It allows a fertility specialist to look directly inside the uterus to identify hidden barriers that ultrasounds often miss, serving as the "GPS" for your entire future treatment plan.
At Shree IVF Clinic, we view a well-performed hysteroscopy not just as a procedure, but as a fundamental step toward a successful pregnancy.
Why Hysteroscopy is Essential for Your Journey?
While blood tests and ultrasounds provide valuable data, they only offer an indirect view of the "soil."
Hysteroscopy stands out because it provides an adequate, real-time diagnosis of the endometrial cavity.
By seeing the environment firsthand, we can decide exactly which specialized tests or treatments—such as MUM-1 markers for infection or corrective surgery—are truly needed.
The "Office Hysteroscopy" Experience
Many patients fear that "surgery" means a long hospital stay. At our clinic, we have streamlined this into a patient-friendly experience:
- No Anesthesia Required: We typically perform this in an "office setting." It is so gentle that most patients do not require any form of anesthesia.
- Quick Recovery: The procedure is very fast. You can typically go home within two hours of arriving at the clinic.
- Widespread Availability: This procedure is easily accessible across India. You can often have it done in your hometown and bring the findings to a referral specialist.
Dr. Jay Mehta’s Advice: Always ask your doctor for a high-quality video recording of your hysteroscopy. Having this record is vital for your future care.
If you move to a referral unit like ours, that video allows us to see exactly what is happening inside your uterus without necessarily repeating the procedure.
How Does Hysteroscopy Change the Treatment Plan?
A hysteroscopy does more than just "look"; it dictates the strategy for your next embryo transfer. Based on the visual findings, we can immediately pivot to:
1. Guided Biopsies: Taking tissue samples from specific "strawberry patches" to test for silent chronic inflammation.
2. Structural Correction: Identifying and planning for the removal of polyps, fibroids, or adhesions (Asherman's Syndrome).
3. Calibrating Transfers: Ensuring the cavity is perfectly "quiet" and healthy before we use your precious frozen embryos.
Take Action: Don't go into your next IVF cycle blindly. Ensure your "soil" is ready for the "seed." Call 1800-268-4000 to know more about how we use hysteroscopy to solve RIF.
Practical Tips for Patients Considering Hysteroscopy
If you are advised to undergo a hysteroscopy, keep these practical points in mind to ensure you get the most value from the procedure:
- Request the Video: As mentioned, the video record is more valuable than a printed report. Ensure you have a digital copy of your medical records.
- Timing Matters: Usually, the best time to perform a diagnostic hysteroscopy is just after your period ends, when the lining is thin and easy to evaluate.
- Minimal Downtime: Since this is an office procedure, you do not need to take multiple days off work. It is a "walk-in, walk-out" diagnostic step.
As a specialist in reproductive medicine, I have seen how a simple 10-minute hysteroscopy can reveal the answer to years of unexplained failure.
My goal is to give you a clear, visual diagnosis so that we can move forward with a plan that actually works.
Stop guessing why your transfers are failing. Let’s take a direct look and find the solution together. Consult with Dr. Jay Mehta at Shree IVF Clinic for a comprehensive hysteroscopic evaluation.
Could an Imbalanced Endometrial Microbiome Be Causing My Recurrent Implantation Failure?
Yes—but not in the way many expensive tests suggest.
The endometrial microbiome refers to the community of "good bacteria" (primarily Lactobacillus) living within your uterine lining.
While a healthy microbiome is essential for an embryo to "stick," testing for it through expensive biopsies is often unnecessary.
Because the concentration of microbes in the uterus is so low, these tests are frequently unreliable.
Instead of focusing on costly uterine “mapping,” a more practical and scientifically grounded strategy is to improve the gut–pelvis axis and eliminate visible infections in the cervix or vagina.
What Is the Endometrial Microbiome?
The endometrial microbiome refers to the small population of beneficial bacteria inside the uterine lining.
In an ideal environment:
-
Lactobacillus species dominate
-
Harmful bacteria remain minimal
-
Local immune balance is stable
-
Implantation signals function smoothly
When this balance is disturbed, inflammation can develop—even without obvious symptoms
Why Is Testing the Uterine Microbiome So Difficult?
While the vaginal microbiome is well-understood, the uterus is a "low-biomass" environment. This means the number of microbes present is tiny, making it very difficult to capture them in a biopsy and grow them in an incubator.
At Shree IVF Clinic, we advise caution before spending resources on expensive microbiome mapping tests.
These investigations often fail to provide a clear clinical benefit because the technology is still catching up to the research.
The Gut–Pelvis Axis: The More Practical Approach
One of the most important emerging concepts in reproductive science is the Gut–Pelvis Axis.
There is a biological connection between gut microbiota, vaginal flora, and the endometrial environment.
Healthy gut bacteria can influence the reproductive tract through immune modulation and bacterial translocation pathways.
The Gut-Pelvis Axis: Why Oral Probiotics Are Often Preferred
One of the most important breakthroughs in reproductive science is the discovery of the gut-pelvis axis.
Research increasingly suggests:
- Oral probiotics improve systemic immune balance.
- Healthy gut bacteria can "transmigrate" and help seed the vaginal environment.
- Vaginal probiotics may provide temporary local benefit but do not correct systemic imbalance.
If the gut microbiome is unstable, the uterine environment may remain vulnerable.
Expert Tip: Don't rush into an expensive ₹40,000 biopsy to "map" your bacteria. A high-quality, 90-day course of oral probiotics is often a more scientifically sound and cost-effective way to prepare your lining for implantation.
Consult with Dr. Jay Mehta to discuss a microbiome-friendly prep for your next transfer.
The Overlooked Role of the Cervix in Implantation
A distorted microbiome is often caused by "ascending infections"—bacteria traveling upward from the cervix or vagina. This is why a thorough physical examination is vital.
- Cervical Health: An unhealthy or infected cervix acts as a gateway for bad bacteria to enter the uterus, causing chronic inflammation (endometritis).
- Vaginal Infections: Even a "minor" yeast or bacterial infection in the vagina can disturb the delicate balance of the endometrium.
At our clinic, examining the cervix is a mandatory part of the first consultation for any patient facing recurrent failure.
It is a simple step, but it is frequently missed in the rush toward high-tech IVF.
Take Action: Have you had a physical examination of your cervix recently? Treating a simple cervical infection can sometimes be the key to fixing "unexplained" failure. Book a comprehensive fertility examination at Shree IVF Clinic, Ghatkopar, Mumbai.
Practical Steps to Balance Your Internal Environment
If you are worried that an "unhealthy" environment is causing your transfers to fail, follow these practical steps:
- Prioritize Oral Probiotics: Start a specialized probiotic supplement at least 2–3 months before your scheduled transfer.
- Treat Infections First: Ensure any vaginal discharge or cervical redness is treated with antibiotics before you attempt an embryo transfer.
- Save Your Resources: Avoid "add-on" microbiome biopsies unless there is a very specific research-based reason provided by your specialist.
As a specialist in reproductive health, I believe in focusing on the basics that actually move the needle.
Restoring the gut-pelvic axis and ensuring the cervix is healthy are simple, low-cost interventions that have a massive impact on your success rates.
Stop searching for answers in expensive tests that lack clinical proof. Let's focus on the proven science of a healthy microbiome to give your embryo the best possible start.
Are Immune Problems Really Causing My Recurrent Implantation Failure—Or Is It Overdiagnosed?
Yes, immune factors can cause recurrent implantation failure (RIF)—but they are far less common than they are marketed to be.
Immune-mediated rejection occurs when the body’s defense system mistakenly identifies an embryo as a foreign threat, preventing implantation.
While immunological factors like antiphospholipid syndrome (APS) are real, they should only be investigated after a confirmatory ultrasound proves the pelvic structure is normal.
Most immune issues can be resolved with simple, affordable treatments; however, patients must be wary of aggressive, expensive therapies that lack significant clinical proof.
Identifying the True "Immune Mismatch"
At Shree IVF Clinic, we follow a structured diagnostic path. We only move toward immune testing once we are certain the "soil" (uterus) and "seed" (embryo) are healthy.
Certain biological conditions can indeed spoil the endometrial microenvironment:
- Antibody Interference: Conditions like Antiphospholipid Syndrome (APS), Anti-nuclear antibodies, and Anti-cardiolipin antibodies can trigger tiny blood clots or inflammation that block implantation.
- HLA Concordance: A "mismatch" or specific similarity in human leukocyte antigens between the couple.
- Absence of Blocking Antibodies: When the mother's body fails to produce the necessary protective response to "shield" the embryo from her immune system.
Dr. Jay Mehta’s Advice: In India, immune therapies are often grossly commercialized and given after just one failed cycle without justification. I urge you to do your research. Most immune issues don't need 'magic' drugs—they need the right diagnosis.
Treatment: From Basic Modulation to Reserve Drugs
The vast majority of immune causes are highly treatable with simple protocols. We categorize treatment into three tiers based on the severity of the immune response:
1. Basic Modulation (Most Common): Low-dose Aspirin and injections of low molecular weight heparin (LMWH). In many cases, we also use Prednisone (steroids) or Hydroxychloroquine (HCQS) to stabilize the environment.
2. Advanced Resistance: If basic treatments fail, we may use Intralipid injections to help calm the endometrial immune response.
3. Reserve Drugs (Rare Situations): For highly specialized cases, we may consider Tacrolimus, Thymosin Alpha, or IVIG. These are "reserve" options and are not used routinely.
The Truth About LIT (Lymphocyte Immunization Therapy)
LIT involves using paternal white blood cells to "prime" the mother's immune system. It is often marketed as a cure-all, but the data tells a different story:
- When it's used: Only in very rare situations (less than 10% of cases) where there is a persistent CDC cross-match.
- The Success Rate: The clinical benefit of LIT is less than 10% in terms of increasing pregnancy rates.
- Our Stance: Because the benefit is so marginal, we do not use LIT therapy aggressively. We believe in transparency—patients should know the low success rate before consenting to this procedure.
Practical Steps Before Considering Immune Treatment in Mumbai, India
If you suspect your immune system is playing a role in your IVF failures, follow these practical steps to protect your health and your finances:
- Confirm the Basics First: Ensure you have had a high-quality ultrasound and hysteroscopy before blaming "immunity."
- Test for the "Big Three": Focus on APS, Anti-cardiolipin, and Anti-nuclear antibodies before moving to more exotic tests.
- Start Simple: Most patients succeed with simple Aspirin and Heparin protocols; don't jump to IVIG therapy or LIT without a clear, documented medical need.
As a specialist in reproductive medicine, my goal is to separate science from marketing.
Immunotherapy should be a targeted tool, not a random "add-on." We focus on protecting your embryo by creating a peaceful, receptive environment through calculated medical intervention.
Don't let commercialized "immune protocols" distract you from the real cause of your failure.
Let’s look at your case with clinical honesty and scientific precision. Connect with Dr. Jay Mehta at the Best Reproductive Immunology Center in Mumbai, India, for a Truthful Review of Immune Factors in RIF
The Role of NK Cells in Implantation: Balancing Your Immune Response
Natural Killer (NK) cells are not the enemy of pregnancy—they are essential for implantation, provided they are present in the right balance.
In reproductive medicine, we specifically focus on uterine NK cells (uNK cells). These are highly specialized immune cells inside the endometrium that help regulate implantation and early placental development.
The key is balance—not elimination.
Understanding the Difference: Peripheral vs. Uterine NK Cells
It is a common misconception that all "natural killer" cells are harmful. In fertility, we must distinguish between the two types:
- Peripheral NK Cells: Found in your bloodstream, these are part of your general immune system.
- Uterine NK Cells (uNK): These are the stars of the implantation process. They do not "kill" the embryo; instead, they are responsible for spiral arterial development—the process of creating the blood vessels that provide oxygen and nutrients to the growing fetus.
The Molecular "Handshake": HLA-C and KIR Receptors
Implantation is a complex molecular dialogue. The embryo expresses a specific protein called HLA-C, which interacts with the KIR receptors on your uterine NK cells.
- If this "handshake" is successful, the embryo implants.
- If the interaction is poor, the embryo may be rejected.
This delicate balance is influenced heavily by your hormones (Estrogen and Progesterone) which act as the fuel for uNK cell development and growth.
Diagnosing NK Cell Issues: The 10–30% Rule
At Shree IVF Clinic, we don't guess—we test. We perform an endometrial biopsy specifically between Day 17 and Day 22 of your menstrual cycle to check the concentration of these cells.
| uNK Cell Concentration | What it Means | Potential Impact |
|---|---|---|
| Below 10% | Often seen in immunocompromised patients. | Poor blood vessel development; failed implantation. |
| 10% to 30% | Optimal Range | Ideal environment for a healthy pregnancy. |
| Above 30% | Overly active / exaggerated inflammation. | Often caused by silent Chronic Endometritis; hostile to embryos |
Dr. Jay Mehta’s Advice: Don't be afraid of the term 'Killer Cells.' In the uterus, these cells are your embryo's best friends, provided they are in the right concentration.
If they are too low, we boost them with immunomodulators; if they are too high, we quiet the inflammation.
Handling Overactive or Underactive uNK Cells
If your tests show an imbalance, we use targeted treatments to restore the "peace" in your uterus:
- For Overactive Cells: High uNK activity is usually a sign of Chronic Endometritis (inflammation). We treat this with a specific course of antibiotics followed by a long course of probiotics to normalize the immune response.
- For Underactive Cells: If cells are reduced, we use immunomodulators to boost your local uterine immunity and encourage the establishment of a healthy lining.
Take Action: Have you had multiple failed transfers with "perfect" embryos? It might be an immune coordination issue. Schedule a specialized uNK cell biopsy with Dr. Jay Mehta in Mumbai
Practical Next Steps for Your Success
If you are investigating recurrent implantation failure, follow these steps to ensure your NK cells are working for you, not against you:
- Time Your Test Correctly: Ensure any biopsy for NK cells is done during the "Luteal Phase" (Day 17-22) for accurate results.
- Look for the Root Cause: If NK cells are high, don't just take steroids—find out if a silent infection (Endometritis) is the real trigger.
- Optimize Hormones: Ensure your progesterone levels are well-supported, as uNK cells depend on these hormones to function.
As a specialist in reproductive medicine, I focus on the intricate "molecular play" that determines your success. We don't just look for a positive pregnancy test; we look to create a sustainable environment where your baby can thrive from day one.
Is your immune system in sync with your embryo? Let’s evaluate your uterine NK cell activity to find the balance you need for a successful pregnancy.
Are Immune Tests Necessary in Recurrent Implantation Failure (RIF)?
Immune tests are necessary in Recurrent Implantation Failure (RIF), but only as a "final step."
They should only be performed after structural issues, embryo quality, and hormonal factors have been ruled out.
Testing must focus on the uterine environment rather than just peripheral blood to be truly accurate.
When Should Immune Testing Be Considered?
At Shree IVF Clinic, we follow a rigorous diagnostic sequence. We do not jump into immune testing immediately because it can lead to unnecessary treatments.
Before we recommend an immune panel, we must have:
- Structural Confirmation: Evidence via high-quality ultrasound or hysteroscopy that the pelvis and uterine cavity are absolutely normal.
- Exclusion of Other Factors: Ruling out chronic infections, thin endometrium, or poor embryo quality first.
What Specific Tests Actually Matter?
While the market is flooded with "exotic" immune tests, we focus on a specific, evidence-based panel that directly impacts clinical decisions:
- Autoimmune Markers: Testing for Anti-nuclear antibodies (ANA), Antiphospholipid antibodies (APLA), and Anti-cardiolipin antibodies. These help us identify if the body is creating "clots" or inflammation that prevents the embryo from attaching.
- Couple Compatibility: HLA typing of both partners and a CDC cross-match to check for biological "mismatches" that might trigger an immune rejection.
- Endometrial Immune Profiling: This is our most critical diagnostic tool. Instead of relying on peripheral blood (which doesn't always reflect what's happening in the womb), we take a biopsy between Day 17 and Day 22 of the menstrual cycle.
Dr. Jay Mehta’s Advice: We are predominantly reliant on the uterine microenvironment, not peripheral blood.
A blood test might say one thing, but the microscopic factors inside the endometrium at the moment of implantation tell the true story. This is why a timed biopsy is indispensable."
Why We Avoid "Complex" or Excessive Testing
There are dozens of highly complex immune tests available today, but we do not recommend them for most patients.
Over-testing often leads to "over-treating" with heavy medications that have significant side effects.
By focusing on Endometrial Immune Profiling, we can look at:
- The exact concentration of immune cells in the lining.
- The microscopic factors responsible for the "dialogue" between the embryo and the mother.
Practical Next Steps for Patients
If you are considering immune testing after multiple failures, keep these three points in mind:
- Timing is Everything: If you are doing a uterine biopsy for immune profiling, ensure it is done exactly between Day 17 and 22 of your cycle (the luteal phase).
- Focus on the Uterus: Prioritize tests that look at the endometrial environment over general blood tests.
- Structure First: If you haven't had a hysteroscopy yet, do that before you spend money on an immune panel.
As a specialist in complex fertility cases, my goal is to provide a diagnosis that leads to a cure, not just more questions.
Immune testing, when used correctly and cautiously, can be the final piece of the puzzle that helps us calibrate your next transfer for success.
Is your immune system the missing link in your fertility journey? Let’s conduct a targeted, scientific evaluation to find out.
Can Thrombophilia Cause Recurrent Implantation Failure (RIF)?
Yes, but it is rare, predictable, and highly manageable when treated with precise dose calibration.
Thrombophilia is a condition where the blood has an increased tendency to clot.
In fertility treatment, excessive clotting can interfere with the delicate blood supply required for embryo implantation.
However, with correct planning and specialist coordination, outcomes are usually excellent.
Why Thrombophilia is a "Predictable" Challenge
In most cases, a patient with a significant thrombophilia is already aware of their condition long before they start IVf treatment
Usually, a clotting event (thrombosis) earlier in life would have already led to a diagnosis and the use of anticoagulant medications.
If you have a known thrombophilia, fertility treatments are generally safe, provided you are managed meticulously.
The "secret" to success isn't just taking blood thinners; it is the precise timing and dosage of those medications before and during the embryo transfer.
The Power of Multidisciplinary Management
At Shree IVF Clinic, we don't manage thrombophilia in isolation. Because these cases involve complex blood dynamics, we work in close coordination with a specialized team:
- Hematologists: To confirm the specific clotting risks and provide the medical "clearance" to proceed with fertility treatments.
- Cardiologists: This is a unique strength of our unit. Our cardiology team works with us before the embryo transfer to calibrate the exact dosage of anticoagulants.
- Dosage Precision: We use Low Molecular Weight Heparin (LMWH) in therapeutic or thrombolytic doses. When monitored correctly, these do not significantly increase the risk of bleeding during pregnancy but do ensure the embryo has the stable blood supply it needs to implant.
As explained by Dr. Jay Mehta, managing RIF with thrombophilia is actually quite simple once the dose correction is correctly established.
We don't guess the dosage; we calibrate it with our cardiology team to ensure the environment is perfect for the embryo. When the dose is right, the outcomes are usually excellent.
How Incorrect Monitoring Leads to Failure?
When the anticoagulant dose is not monitored or calibrated to the patient's specific biological needs, the tiny blood vessels in the uterine lining can develop microscopic clots. These clots act as physical and biological barriers:
- Nutritional Blockage: They block the essential nutrients from reaching the embryo.
- Failed Synchronization: They prevent the molecular "handshake" between the embryo and the lining.
- Early Loss: They lead to repeated failures or very early miscarriages.
By having a dedicated cardiology team on-site, we eliminate this guesswork. Once they calibrate the dose for your specific body weight and medical history, the "hostile" clotting environment is neutralized.
Practical Next Steps for Your Journey
If you are a patient with a known clotting disorder heading into an embryo transfer, follow these steps:
- Get Specialist Clearance: Ensure your hematologist and fertility specialist are in direct communication.
- Pre-Transfer Calibration: Do not wait for a positive pregnancy test to start or adjust your blood thinners; the dosage should be set before the embryo is transferred.
- Trust the Monitoring: Regular blood monitoring is essential to ensure your anticoagulant levels stay within the "safe zone"—effective enough to prevent clots but controlled enough to avoid bleeding.
As a specialist in complex RIF cases, I believe that high-risk conditions like thrombophilia require a high-precision team.
We combine reproductive science with cardiology expertise to turn a high-risk situation into a successful pregnancy.
Thrombophilia shouldn't be a barrier to your parenthood. Let’s work with our specialists to find the exact dose your body needs for a successful implantation.
When Are Blood Thinners Justified in Recurrent Implantation Failure (RIF)?
Blood thinners, such as Low Molecular Weight Heparin (LMWH), are no longer considered a "blanket benefit" for all IVF patients.
Their usage must be strictly justified by medical history or specific diagnostic markers; using them empirically (without proof) adds unnecessary physical and financial burden to the patient.
The Ethical Challenge of "Pharmacy-Driven" Treatment
In many for-profit fertility establishments across India, blood thinners are often prescribed to every patient simply to "jack up" pharmacy sales.
This is an unethical practice where patients are sometimes forced to purchase expensive injections from the clinic's own pharmacy without a clear medical indication.
At Shree IVF Clinic, we strongly believe that treatment must be evidence-based. Because regulatory backup in India is often limited, it is up to the patient and ethical practitioners to ensure that drugs like Heparin are only used when they truly move the needle for success.
When is Low Molecular Weight Heparin (LMWH) Justified?
While we avoid empirical use, LMWH is a life-changing intervention for a specific group of patients. It is justifiable in a patient who meets any of the following criteria:
- Repeated Obstetric Failures: A history of multiple IVF failures, multiple previous abortions, or preterm births.
- Maternal Age: Patients over the age of 38, where the vascular environment may need more support.
- Past Pregnancy Complications: A history of pre-eclampsia (high blood pressure during pregnancy).
- Abnormal Blood Flow: Elevated Uterine Artery PI (Pulsatility Index) detected during an early pregnancy scan, indicating resistance in blood flow to the uterus.
- Confirmed Thrombophilia: Any clotting disorder where a hematologist has explicitly recommended anticoagulation.
Dosage and Administration: A Specialized Approach
For prophylactic use (prevention), LMWH is typically administered as a subcutaneous injection (under the skin) at a dose of either 40 mg or 60 mg.
- Multidisciplinary Calibration: We do not guess the dose. The specific requirement for your body is best decided in combination with a cardiologist. This ensures the dose is high enough to be effective but low enough to remain safe for the mother.
- Timing: When justified, the administration often begins around the time of the embryo transfer to ensure optimal blood flow during the critical implantation window.
Dr. Jay Mehta’s Advice: Don't accept a prescription for blood thinners just in case. 'If your doctor cannot provide a clinical justification based on your age, history, or blood flow scans, you are likely being overtreated.
Precision in medicine means giving the right drug to the right patient, not every drug to every patient.
Next Steps for Your Journey
If you are being advised to use blood thinners for your next cycle, follow these steps to ensure it is the right move for you:
- Ask for Justification: Ask your consultant which specific factor (Age, PI index, or Thrombophilia) justifies the use of Heparin in your case.
- Check the Uterine Artery PI: Ensure your clinic performs a Doppler scan of the uterine arteries during your preparation; this is a key indicator of whether blood thinners are actually needed.
- Seek Cardiology Input: If you are prescribed a 60 mg dose, ensure a cardiologist has reviewed your cardiovascular health to confirm the safety of that dosage.
As a specialist committed to ethical fertility care, I focus on protecting my patients from unnecessary interventions. Blood thinners are a powerful tool, but they must be used as a scalpel, not a sledgehammer.
Are you being prescribed "add-on" injections without a clear reason? Let’s review your history and scans to see if blood thinners are truly necessary for your success. Visit our Shree IVF Clinic in Mumbai for an ethical review of your IVF protocol.
Are Immune Therapies Being Overused in IVF?
Immune therapies are some of the most over-prescribed and abused treatments in Indian fertility care.
In many commercial clinics, they are given "blindly" after a single failure without ruling out structural pelvic issues or embryo quality.
This practice not only adds unnecessary financial burden but can also lead to medical frustration when the underlying cause of failure remains unaddressed.
The "Embryo and Pelvis First" Rule
At Shree IVF Clinic, we follow a strict medical hierarchy. Reproductive immunology is a valid science, but its foundation rests on two non-negotiable prerequisites:
1. A Clean Pelvis: You cannot blame "immunity" if you have untreated Endometriosis, Fibroids, or Adenomyosis. These structural issues must be resolved first.
2. A Normal Embryo: Ideally, the embryo should be genetically tested (PGT-A) to ensure the failure isn't simply due to chromosomal issues.
Unfortunately, many Indian patients are subjected to immunotherapy despite having visible pelvic pathology.
When the treatment inevitably fails, they lose hope, not realizing the therapy was never indicated for them in the first place.
The Abuse of LIT and Intralipids
Two of the most frequently misused therapies in India are:
- Paternal Lymphocyte Immunization Therapy (PLIT): This is often performed after just one abortion or one IVF failure without proper evaluation. Scientifically, PLIT has very narrow indications and should never be a first-line "add-on."
- Intralipid Injections: These are often injected into patients without any prior testing for immune activity (like uNK cell concentration).
Reserve Therapies: Use with Extreme Caution
There are powerful drugs available for true immune-mediated rejection, but they are "reserve therapies" and must be used sparingly:
- Tacrolimus, IVIG, and Thymosin Alpha: These treatments have very specific indications in reproductive immunology. For example, IVIG (Intravenous Immunoglobulin Therapy) in Mumbai, India, is sometimes used in patients with confirmed immune-related implantation failure or recurrent pregnancy loss after detailed evaluation.
Similarly, Thymosin Alpha is reserved for patients who have experienced multiple biochemical pregnancies or recurrent miscarriages despite high-quality embryo transfers.
- Safety Verification: Some of these immune-modulating medications can affect kidney function and overall immune balance. For this reason, when therapies such as IVIG infusion therapy for recurrent IVF failure are considered, our protocols are often reviewed in collaboration with a nephrologist to ensure that the patient’s renal health remains completely safe
At our center, immune therapies like intravenous immunoglobulin therapy, tacrolimus, or other immunology treatments are never used as routine IVF add-ons.
They are only recommended after careful immune testing, pelvic evaluation, and embryo quality assessment.
Dr. Jay Mehta’s Advice: Don't say 'yes' to immune modulation just because you are frustrated.
If your clinic recommends Intralipids or PLIT after a single failure without looking at your pelvis or embryo genetics, seek a second opinion. Immunity is a complex lock; you cannot open it with a random key.
Why Consult a Reproductive Immunologist?
If you are navigating Recurrent Implantation Failure (RIF), we strongly encourage you to consult a specialist in this field before starting treatment.
- Accessibility: Most reproductive immunologists offer online consultations, meaning you can access expert care from your own city without logistical hurdles.
- Evidence-Based Care: A specialist will ensure you only take what you need, protecting you from the risks of over-medication.
Book an Online Consultation with our Reproductive Immunology team
Next Steps for Your Journey
If immunotherapy has been suggested to you, take these three steps to protect your health:
- Demand a Structural Audit: Ensure your doctor has ruled out adenomyosis and endometriosis via a high-quality 3D scan or hysteroscopy first.
- Ask for the Data: If PLIT or IVIG is suggested, ask for the specific test results (like HLA typing or CD138/MUM-1) that justify its use.
- Check Your Kidney Health: If you are prescribed reserve drugs like tacrolimus, ask for a baseline renal function test (KFT) to ensure your body can handle the medication.
As a referral unit for complex RIF, my goal is to stop the cycle of "blind" treatments. Immunotherapy is a scalpel that must be used with precision.
We focus on healing the pelvis and selecting the best embryo before we ever consider modulating your immune system.
Are you being offered "blanket" immune treatments for your IVF failures? Let’s conduct a truthful, targeted evaluation to see what your body actually needs.
Consult with Dr. Jay Mehta at Shree IVF Clinic for a truthful review of your immune protocol.
Can Sperm Cause Recurrent Implantation Failure?
Yes, sperm quality is a critical—and often overlooked—factor in recurrent implantation failure (RIF).
While fertility treatment frequently focuses on the female partner, sperm contributes 50% of the embryo’s genetic material.
If sperm integrity is compromised, the embryo may appear morphologically “normal” in the lab but still fail to implant or result in an early biochemical pregnancy.
Implantation is not just about embryo appearance—it is about genetic integrity.
Moving Beyond the "Normal" Semen Report
One of the biggest mistakes in fertility practice is assuming that a standard semen analysis tells the whole story.
A report might show a "normal" count and motility, but a deeper evaluation often reveals hidden issues:
- Abnormal Morphology: The poor shape of the sperm affects its ability to penetrate the egg and carry out the early stages of embryo growth.
- Liquefaction Issues: Problems with how the semen transitions from a gel to a liquid can indicate underlying prostate or enzyme issues that affect sperm health.
- The DNA Fragmentation Index (DFI): This is the most vital advanced test. It measures the "breaks" in the genetic material within the sperm head. High DNA fragmentation is a leading cause of embryos that fail to implant or result in early chemical pregnancies.
The "Male Biological Clock": Age and Integrity
It is a common myth that only a female's age matters. We must categorically understand that the male partner's age is also a decisive factor:
- The Age 45 Milestone: Typically, after the age of 45, sperm DNA begins to deteriorate significantly, even if the count and motility remain stable.
- Embryo Quality: "Older" sperm is more likely to contribute to genetic errors in the embryo, leading to RIF or repeated miscarriages.
Dr. Jay Mehta’s Advice: In my practice, I insist on undivided attention for the male partner. You cannot solve a 50/50 problem by only looking at one side.
If you have experienced repeated failures, we must test the 'integrity' of the sperm, not just the ''count."
Restoring Sperm Health: Lifestyle and Therapy
Fortunately, unlike eggs, sperm are constantly being produced, which means we can often improve their quality through targeted interventions:
- Lifestyle Modifications: Reducing heat exposure (saunas, laptops), quitting smoking, and managing stress can significantly lower DNA fragmentation.
- Anti-Oxidation Therapy: The administration of specific, high-dose antioxidants can help repair oxidative stress damage to the sperm membrane and DNA.
- Advanced Selection: In cases of high DFI, we use advanced sperm selection techniques like MACS (Magnetic-Activated Cell Sorting) or Microfluidics to ensure only the healthiest sperm are used for Intracytoplasmic Sperm Injection (ICSI)
Take Action: Has your partner only had a basic semen analysis? Schedule an advanced Sperm DNA Fragmentation (DFI) test at Shree IVF Clinic
Practical Next Steps for the Male Partner
If you are navigating the frustration of RIF, ensure the following steps are taken for the male partner:
- Request a DFI Test: Do not rely on a basic semen report; ask for a DNA Fragmentation Index.
- Review Age Factors: If the male partner is over 45, start antioxidant therapy at least 3 months before the next IVF cycle.
- Check for Varicocele: A physical examination by a specialist can rule out enlarged veins in the scrotum, which are a common (and fixable) cause of high DNA fragmentation.
As an expert in recurrent implantation failure & male infertility treatment in Mumbai, India, I believe in treating the couple as a unit.
By improving sperm integrity, we improve the "blueprint" of the embryo, giving it a much higher chance of sticking and growing into a healthy baby.
Is the male factor the missing piece of your fertility puzzle? Let’s conduct a comprehensive evaluation of sperm integrity to ensure your next cycle is your last. Consult with Dr. Jay Mehta at Shree IVF Clinic for a truthful male fertility evaluation.
Can High DNA Fragmentation Cause Recurrent Implantation Failure (RIF)?
Yes—sperm DNA Fragmentation Index (DFI) is one of the most overlooked yet critical factors in embryo success.
While an embryo may look "perfect" under a microscope, high DNA fragmentation can lead to poor development and recurrent implantation failure (RIF).
Identifying and treating high DFI is one of the most effective ways to break the cycle of failed transfers.
What Is the DNA Fragmentation Index (DFI)?
While a standard semen analysis looks at the "external" factors (count, basic morphology, and motility), the DFI test looks at the "internal" genetic integrity.
It measures the percentage of sperm that have damaged or broken DNA strands.
- DFI < 15%: This is considered a good, healthy range for successful implantation.
- DFI > 25%: This warrants immediate medical intervention and lifestyle modification, as it significantly reduces the chances of a successful pregnancy.
At Shree IVF Clinic, this is a routine part of our advanced semen analysis. The test is highly convenient for the male partner—it takes only four hours for the results and can be performed irrespective of abstinence.
Why Does High DFI Lead to Implantation Failure?
When a sperm with high DNA fragmentation fertilizes an egg, the resulting embryo often carries genetic "breaks." This leads to:
- Early Developmental Arrest: The embryo stops growing before it can implant.
- Failed Implantation: The embryo may reach the uterus but lacks the genetic "engine" to attach and grow.
- Chemical Pregnancies: Very early miscarriages shortly after a positive test.
High DFI does not always prevent fertilization—it disrupts development after fertilization.
Why Does DNA Fragmentation Increase?
Common causes include oxidative stress, smoking, obesity, heat exposure (saunas, laptops, tight clothing), varicocele, and advanced paternal age.
After age 45, DNA fragmentation rates tend to rise even if count and motility remain normal.
When Lifestyle Changes Are Not Enough: The TESE/TESA Option
The good news is that sperm is produced in cycles, meaning high DFI is often reversible. We typically recommend a three-month protocol focusing on:
1. Lifestyle Modifications: Reducing exposure to heat (laptops, saunas), quitting smoking, and managing weight.
2. Anti-oxidation Therapy: High-dose antioxidants to reduce oxidative stress, which is the primary cause of DNA damage.
Dr. Jay Mehta’s Advice: Visible benefits in DFI are usually seen after three months of consistent lifestyle changes.
We don't just jump to advanced procedures; we give the body time to produce healthier, higher-integrity sperm first.
Using testicular sperm for ICSI can sometimes improve outcomes in selected RIF cases.
The "Testicular Sperm" Breakthrough
In some situations, the DFI remains persistently high despite three months of treatment.
If a couple has already experienced implantation failure with good-looking embryos, we consider a more advanced surgical approach:
- TESE/TESA (Testicular Sperm Extraction): Sperm collected directly from the testicles often has significantly lower DNA fragmentation than sperm found in the ejaculate. This is because much of the DNA damage occurs as sperm travels through the reproductive tract.
- Why it works: By using testicular sperm for ICSI, we bypass the area where most DNA "breaks" happen, providing the best possible genetic blueprint for the embryo.
Take Action: If you have had "Grade A" embryos fail to implant, the answer may lie within the sperm DNA. Schedule an advanced DFI test at Shree IVF Clinic to evaluate your embryo's blueprint.
Practical Next Steps for the Male Partner
If high DFI is suspected, follow these steps to optimize your next cycle:
- Don't Wait for the Day of Retrieval: Test your DFI well in advance so you have the three-month window required for improvement.
- Cool Down: Avoid tight clothing and heat exposure to the scrotum, as heat is the biggest enemy of sperm DNA.
- Consult an Andrologist: If your DFI is over 25%, a specialist can rule out physical issues like a varicocele that may be causing the damage.
As a specialist in RIF, I believe that half of the embryo's success belongs to the male partner.
We use science to look beneath the surface and ensure that every embryo we transfer has the genetic strength to become a healthy baby.
Is high sperm DNA fragmentation the silent cause of your IVF failures? Let’s identify the truth and restore your path to success.
Is Male Factor the Hidden Reason Behind Your Repeated IVF Failures?
Yes—male factor infertility can directly affect embryo survival, not just fertilization.
The sperm’s responsibility does not end at fertilizing the egg. It plays a decisive role in embryonic genomic activation, the stage that determines whether an embryo continues developing or stops growing.
If the sperm quality is poor, it can cause high levels of fragmentation within the embryo, leading to repeated failure even if the initial fertilization seemed successful.
What Happens During Embryonic Genomic Activation?
A common misconception is that once an egg is fertilized, the male's job is done. However, between the third and fifth day of development, the embryo undergoes embryonic genomic activation.
This is the moment the embryo "switches on" its own DNA—half of which comes from the sperm.
- Sperm Quality and Embryo Survival: If the inherent quality of the chosen sperm is poor (due to abnormal morphology or motility), the embryo may struggle to complete this activation.
- The "Fragmentation" Problem: In cases of severe male factor infertility, we often see embryos that begin to break apart or "fragment" internally during these early days. This is a clear indicator that the paternal genetic contribution is compromised.
Time-Lapse Imaging: The Truth in the Incubator
How do we know the male factor is the culprit? At Shree IVF Clinic, we use Time-Lapse Imaging (Embryoscope).
This technology allows us to watch the embryo's development every minute without removing it from the incubator.
- Tracking the Timeline: By observing the exact timing of cell division, we can identify "paternal stress" on the embryo.
- Early Detection: If an embryo starts fragmenting specifically after day 3, it points strongly toward a male factor issue rather than an egg issue.
Dr. Jay Mehta’s Advice: If you have had multiple cycles where embryos 'collapsed' or fragmented after day 3, we must stop blaming the egg and look at the sperm.
The sperm provides the 'engine' for the embryo's growth. If the engine is faulty, the embryo won't reach the finish line.
Correcting the Male Factor Before the Next IVF Cycle
Repeated failure is a sign that the "blueprints" need to be fixed before building again. We focus on two primary strategies:
1. Sperm Selection Technologies: Instead of just picking a "moving" sperm, we use advanced selection tools like MACS (Magnetic-Activated Cell Sorting) or PICSI to ensure we select sperm with the highest genomic integrity and the lowest DNA damage.
2. Addressing Oxidative Stress: High fragmentation in embryos is often caused by oxidative stress in the male partner. We treat this with an intensive 3-month regimen of antioxidants and lifestyle changes to improve the "starting material."
Take Action: Are your embryos failing to reach the blastocyst stage? It may be time for a paternal health audit. Consult with Dr. Jay Mehta to review your embryo development logs
Practical Next Steps for the Couple
When facing repeated IVF failure, the male partner should undergo the following specialized evaluations:
- Embryo Morphokinetic Review: Ask your embryologist for a detailed report on when and how your previous embryos fragmented.
- Advanced Selection Consultation: Discuss the use of MACS or microfluidic sperm sorting to bypass damaged sperm during ICSI.
- Andrology Specialist Visit: Rule out physical factors like varicocele that increase oxidative stress and damage the "paternal engine."
As a specialist in recurrent implantation failure, I believe in equal accountability for the egg and the sperm.
By identifying male-factor fragmentation early through time-lapse technology, we can change our selection strategy and finally achieve a successful, healthy pregnancy.
Is your embryo's "engine" failing? Let’s conduct a deep-dive analysis into the paternal factors affecting your IVF success.
Does Sperm Affect Implantation After ICSI?
Yes, sperm quality significantly affects implantation rates after ICSI.
Even after a successful ICSI (Intracytoplasmic Sperm Injection) procedure where fertilization has occurred, the sperm’s quality remains a deciding factor in whether that embryo will actually implant.
The sperm is responsible for the "genomic shift"—the engine restart of the embryo—which is required to reach the blastocyst stage and achieve a successful pregnancy.
The Genomic Shift: Why "Fertilization" Isn't Enough
Many patients assume that once the sperm is injected into the egg (ICSI) and fertilization is confirmed, the male factor is no longer relevant. This is a scientific misconception.
After the initial stages of cell division, the embryo must undergo a Genomic Shift (also known as Embryonic Genomic Activation).
This is the moment the embryo stops relying on the egg's nutrients and "switches on" its own DNA—50% of which is provided by the sperm.
- The Blastocyst Barrier: If the sperm quality is poor, the embryo often fails this genomic shift. It may look healthy on Day 2 or Day 3 but will stop growing or "arrest" before reaching the Blastocyst stage (Day 5).
- Implantation Success: Only a high-quality blastocyst that has successfully completed this shift has the biological strength to implant in the uterine lining.
Inherent Sperm Quality vs. Visual Selection
During ICSI, an embryologist selects a sperm based on how it looks (morphology) and how it moves (motility). However, "good-looking" sperm can still have internal defects:
- DNA Integrity: High levels of DNA fragmentation can prevent the genomic shift from occurring correctly.
- Centriole Function: The sperm provides the "motor" (centriole) that allows the embryo's cells to divide. If this motor is faulty, the embryo's development will be chaotic.
- Epigenetic Factors: The sperm carries "instructions" that tell the embryo how to interact with the mother’s uterus.
Dr. Jay Mehta’s Advice: ICSI is a great tool, but it isn't a cure for poor sperm biology. If we inject a sperm with damaged DNA, the embryo will likely fail to reach the blastocyst stage or fail to implant.
This is why a complete evaluation of the male partner is non-negotiable before starting any IVF cycle.
The Importance of Comprehensive Male Evaluation
To ensure the best outcomes for implantation, we move beyond the basic semen analysis. At Shree IVF Clinic, we look at the male factor as a primary pillar of success:
- Advanced Diagnostic Testing: We use DNA Fragmentation Index (DFI) testing to check the internal "blueprint" of the sperm.
- Pre-ICSI Optimization: We often put the male partner on a 3-month course of specialized antioxidants and lifestyle modifications to improve the inherent quality of the sperm before the ICSI procedure.
- Sperm Selection Tech: In cases of repeated failure, we use technologies like MACS or Microfluidics to select sperm based on biological health, not just visual appearance.
Take Action: Are your embryos failing to reach the blastocyst stage despite "good" ICSI results? Schedule an advanced male fertility consultation with Dr. Jay Mehta to evaluate the genomic health of your sperm.
Practical Next Steps for Your Journey
If you are preparing for ICSI or have experienced failed implantations, follow these steps:
- Don't Settle for Basic: Ensure the male partner has had a DNA Fragmentation Index (DFI) test.
- Lifestyle Audit: Focus on reducing oxidative stress (no smoking, limited heat exposure, healthy BMI) for at least 90 days before egg retrieval.
- Discuss Blastocyst Culture: Ask your clinic about their blastocyst conversion rates; this is often the best indicator of paternal genomic health.
As a specialist in recurrent implantation failure, I believe that equal attention to the male factor is the key to unlocking better success rates.
By ensuring the sperm is healthy enough to power the genomic shift, we give your embryos the best possible chance of becoming a healthy, successful pregnancy.
Is your sperm quality holding back your IVF success? Let’s conduct a truthful evaluation and build a stronger foundation for your future baby.
Is Advanced Sperm Testing the Missing Link in Recurrent Implantation Failure (RIF)?
Yes—in RIF cases, the most essential advanced sperm test is the DNA Fragmentation Index (DFI).
But testing alone is not enough.
The real breakthrough lies in how we use that information; advanced selection techniques like microfluidic chips allow us to filter out damaged sperm and select only the high-integrity candidates for your embryos.
Why Is DFI the Non-Negotiable Test in RIF?
While standard semen analysis looks at whether sperm can "swim," the DNA Fragmentation Index (DFI) looks at whether they can "build." High DFI means the genetic material inside the sperm head is broken.
- The Impact: Sperm with high fragmentation may still fertilize an egg, but the resulting embryo often stops developing or fails to implant.
- The Threshold: If your DFI is above 25%, it is a significant red flag for RIF and requires a specialized approach in the lab.
The Real Breakthrough: Microfluidic Sperm Selection
Once we identify that a patient has high DNA fragmentation, we don't just proceed with standard ICSI. We utilize the Microfluidic Sperm Sorting Chip—an excellent addition to our IVF laboratory.
How it Works:
Traditional sperm preparation involves "centrifugation" (spinning the sample at high speeds), which can actually cause more oxidative stress and DNA damage.
In contrast, the microfluidic chip mimics the natural path sperm take through the female reproductive tract:
- Natural Selection: Sperm are placed in a tiny channel and must "swim" through microscopic pores.
- Survival of the Fittest: Only the most motile, healthy, and genetically intact sperm can navigate the chip.
- The Outcome: This allows the embryologist to collect a sub-population of sperm with the lowest possible DNA fragmentation index, significantly improving the chances of a healthy blastocyst and successful implantation.
Breaking the Cycle of Failure
In cases of RIF, we use these advanced tools to ensure we aren't just repeating the same mistakes. By combining DFI testing with Microfluidic selection, we move from "random selection" to "precision selection."
Dr. Jay Mehta’s Advice: Advanced testing is useless without an advanced solution. If your DFI is high, the Microfluidic Chip is arguably the most important 'add-on' you can choose. It removes the 'noise' of damaged sperm and gives your egg the best possible genetic partner.
Practical Next Steps for the Male Partner
If you have experienced multiple failed IVF cycles, your advanced sperm strategy should be:
- Test the Blueprint: Perform a DFI test to see if genetic damage is a factor.
- Skip the Centrifuge: If your DFI is high, insist on using a Microfluidic Chip for sperm preparation in your next cycle.
- Optimize for 90 Days: Remember that sperm takes about 3 months to mature; use this time for antioxidant therapy to improve the "raw material" before using advanced selection tools.
As a specialist in RIF, my goal is to provide the most scientifically sound laboratory environment for your embryos. Using microfluidics to manage DNA fragmentation isn't just about "new technology"—it's about ensuring that the 50% of the embryo provided by the father is of the highest possible quality.
Are you ready to stop the cycle of unexplained failures? Let’s use advanced selection technology to find your healthiest sperm and give your embryos a new chance at life.
Could Paternal Epigenetics Be the Hidden Cause of Unexplained Implantation Failure?
Paternal epigenetics refers to the "instructions" on the sperm's DNA that tell the embryo's genes how to behave.
Yes—even when sperm DNA appears structurally normal, the “instructions” carried on that DNA may be faulty.
While we don't yet have a routine clinical test to "map" these markers, we know that factors like male age significantly impact these epigenetic signals, leading to unexplained implantation failure.
What is Paternal Epigenetics?
Think of the DNA as the "hardware" and epigenetics as the "software."
Epigenetics involves chemical tags (like methylation) that sit on top of the DNA. These tags don't change the genetic code, but they control which genes are turned "on" or "off" during the embryo's development.
- The Silent Saboteur: An embryo can appear perfectly normal under a microscope and even pass genetic testing (PGT-A), but if the paternal "software" is glitchy, the embryo may lack the instructions needed to successfully attach to the uterus or develop a functional placenta.
- The Genomic Activation Role: As discussed in previous sections, the sperm is responsible for "restarting" the embryo's engine on Day 3. Epigenetics plays a vital role in ensuring this restart happens correctly.
The Age Factor: Why 45 Is a Biological Milestone
Because we currently lack a "crystal clear" diagnostic test for paternal epigenetics, we rely on clinical indicators. The most significant of these is paternal age.
- The Deterioration Point: In men over the age of 45 years, the epigenetic markers on the sperm begin to degrade.
- The "Invisible" Failure: Even if the semen analysis is "excellent" and the embryos look like "Grade A" blastocysts, the age-related epigenetic changes can cause consistent, repeated implantation failure.
The Future of Diagnosis and Modification
We are currently in a transition period in reproductive science. While we cannot yet pinpoint the exact epigenetic cause for every patient, research is moving rapidly.
- The Next Decade: Within the next 10 years, we expect to see standardized tests that can identify specific epigenetic errors in a sperm sample.
- Modification Potential: Just as we use antioxidants to improve DNA fragmentation, future therapies may allow us to "reset" or modify paternal epigenetic markers through specific nutritional or pharmacological interventions.
Practical Advice for the "Older" Male Partner
If the male partner is over 45 and you have experienced RIF, we recommend the following proactive steps:
- Acknowledge the Biological Clock: Understand that male age is a variable. If embryos are failing despite a healthy female partner, the paternal "software" should be considered.
- Optimize What We Can: Since we cannot test epigenetics directly yet, we focus on minimizing the factors that damage it—such as smoking, obesity, and environmental toxins.
- Advanced Selection: Using tools like Microfluidics can help select sperm that are more likely to have higher biological integrity, even if we cannot see the epigenetic tags themselves.
As a specialist in RIF, I am closely following the research into paternal epigenetics.
It is the "missing link" for many couples with unexplained failure. While we wait for the technology to catch up, we use clinical experience and age-based protocols to give you the best chance of success.
Are you facing "unexplained" failures despite having perfect embryos? Let’s evaluate the paternal factors that might be operating beneath the surface. Consult with Dr. Jay Mehta at Shree IVF Clinic for a deep dive into paternal factors.
Could Insulin Resistance Be the Hidden Metabolic Barrier to Implantation?
Insulin resistance—often seen in patients with PCOS (both thin and lean types) or diabetes—is a significant cause of recurrent implantation failure.
It disrupts the "biological clock" of the uterus, shifting the window of implantation (WOI) and making the lining unreceptive even when embryos are of excellent quality.
How Insulin Resistance Disrupts Implantation?
Insulin is not just a sugar-regulating hormone; it is a master metabolic signal. When your body becomes resistant to insulin, it creates a cascade of hormonal imbalances that directly affect the uterus:
- Shifting the Window of Implantation (WOI): High insulin levels can cause the uterine lining to mature too quickly or too slowly. This means when the embryo is ready to "land," the uterus is either not yet ready or has already closed its doors.
- Inflammatory Environment: Insulin resistance creates a low-grade chronic inflammation in the endometrium, making it a "hostile soil" for the embryo.
- PCOS-Related Complications: In patients with PCOS, insulin resistance is often the root cause of poor egg quality and a displaced implantation window.
The Importance of Concurrent Management
At Shree IVF Clinic, we don't treat infertility in a vacuum. If we detect insulin resistance, your treatment must be twofold:
1. Fertility Strategy: Calibrating the timing of the embryo transfer to account for a potentially shifted window.
2. Endocrine Strategy: We insist that patients stay in close contact with an endocrinologist. Managing the metabolic side is just as important as the IVF side.
Dr. Jay Mehta’s Advice: You cannot out-IVF a metabolic disorder. If your insulin resistance is not controlled, even the most expensive 'Grade A' genetically tested embryo will likely fail. We must stabilize your metabolism first to ensure the uterus is 'quiet' and receptive.
Therapeutic Approaches: From Oral Meds to Insulin
Correcting insulin resistance requires a disciplined, medical approach:
- Oral Therapy: Most patients respond well to oral insulin-sensitizing agents (like metformin) and specific lifestyle modifications (low-carb, high-protein diets and exercise).
- Switching to Insulin: In more severe cases or when oral medications are insufficient, we may recommend switching to insulin injections under the guidance of an endocrinologist to achieve precise control before the transfer.
- Weight Management: Especially in "thick" PCOS, losing even 5–10% of body weight can significantly improve insulin sensitivity and implantation rates.
Practical Next Steps for Your Journey
If you have PCOS or a family history of diabetes and have faced implantation failure, follow these steps:
- Test Your HOMA-IR: Don't just check fasting sugar; ask for a HOMA-IR test (Homeostatic Model Assessment for Insulin Resistance) to see how hard your body is working to manage sugar.
- Stabilize Before Transfer: Aim for at least 2–3 months of stable metabolic markers before attempting your next embryo transfer.
- Endocrinology Review: Ensure your fertility specialist and endocrinologist are aligned on your medication dosages.
As a specialist in complex RIF, I view insulin resistance as a "fixable" barrier.
By addressing the metabolic foundation, we can reset your window of implantation and significantly increase your chances of a successful pregnancy.
Is an undiagnosed metabolic issue the reason your transfers are failing? Let’s conduct a comprehensive endocrine and fertility review to find the answer.
Is PCOS Causing Your Recurrent Implantation Failure?
Yes, PCOS (Polycystic Ovary Syndrome) can cause recurrent implantation failure (RIF). It can create a “quantity vs. quality” trap in IVF.
It produces a high number of eggs with poor internal quality and creates a metabolic environment that severely shifts the window of implantation (WOI), making it difficult for even a good embryo to "stick."
The Paradox of PCOS: Many Eggs, Few Babies
In a typical PCOS IVF cycle, we often retrieve a large number of eggs. However, the success rate doesn't always match the quantity. This is due to several factors:
- The Androgen Environment: PCOS ovaries contain a micro-environment with excessive androgens (male hormones). This "hostile" environment suppresses healthy follicle growth, leading to poor egg quality.
- The Blastocyst Barrier: Because the eggs are of suboptimal quality, we often see a "drop-off" in the lab—many eggs are fertilized, but very few survive to become high-quality blastocysts.
- Genetic Integrity: Even if a blastocyst is formed, it may not have the optimal chromosomal or energetic quality needed for successful implantation.
The "Obese PCOS" Factor and the Window of Implantation
In India, we see a high prevalence of obese PCOS. For these women, the challenge isn't just the eggs; it’s the "soil."
- Altered Receptivity: Excess weight and hormonal imbalances shift the Window of Implantation (WOI). This means the uterus might be "ready" for the embryo at a time that doesn't align with the embryo's development.
- The 10-15% Rule: For obese patients with RIF, we strongly recommend a weight loss of 10 to 15% of total body weight before the next transfer. This is not just for general health; it is a clinical intervention to "reset" the uterine environment and bring the implantation window back to normal.
Flexibility in IVF Stimulation Protocols
One unique aspect of PCOS management is that stimulation for IVF doesn't always have to follow the rigid "Day 2 or 3" rule.
- Any-Day Start: Because the follicles in a PCOS ovary are often heavily suppressed by the internal environment, we can sometimes start stimulation on almost any day of the menstrual cycle.
- Customized Protocols: This flexibility allows us to tailor the cycle to the patient’s specific hormonal profile, which is especially important after a previous failed IVF cycle.
Dr. Jay Mehta’s Advice: PCOS is rampant, but it is manageable. If you have failed multiple times, don't keep doing the same stimulation.
We must focus on improving egg quality through pretreatment and resetting your uterine receptivity through weight management and metabolic control.
Practical Next Steps for PCOS Patients With RIF
If you have PCOS and are facing recurrent failure, consider these focused steps:
- Prioritize Blastocyst Culture: Don't settle for a Day 3 transfer. In PCOS, we need to see which embryos have the strength to reach Day 5 (blastocyst) to ensure they are viable.
- Focus on the "Three-Month Prep": Use 90 days to improve your metabolic health, reduce androgens, and lose a target percentage of weight before your next egg retrieval.
- Metabolic Support: Ensure you are on the right dosage of insulin-sensitizing medications (like Metformin) to help stabilize the uterine environment.
As a specialist in PCOS treatment in Mumbai, India, I treat PCOS as a systemic issue, not just an ovarian one.
By addressing the androgen levels and the metabolic impact on the uterus, we can move from "many eggs" to "one healthy baby."
Is PCOS causing a mismatch between your embryos and your uterus? Let’s create a targeted plan to reset your system for success. Consult with Dr. Jay Mehta for a specialized PCOS and RIF evaluation today
Thyroid Dysfunction and RIF: The Hidden "Switch" for Implantation
Thyroid dysfunction is one of the most common—and fortunately, most treatable—causes of recurrent implantation failure (RIF).
Specifically, the presence of anti-TPO antibodies can create an immune imbalance that prevents an embryo from sticking, even if your TSH levels appear to be in the "normal" range for a non-pregnant person.
The Role of Anti-TPO Antibodies
Many patients are told their thyroid is "fine" because their TSH is under 4.5. However, in fertility medicine, we look deeper.
If you have a high anti-TPO titer (more than 1:40), your body is essentially producing antibodies that attack your own thyroid gland.
- Immune Cross-talk: The presence of these antibodies indicates an overactive immune system. This same immune "aggression" can mistakenly target the embryo, leading to implantation failure or early miscarriage.
- Mandatory Supplementation: At Shree IVF Clinic, we consider thyroid supplementation mandatory for any patient with a titer above 1:40, as it helps stabilize the immune environment and supports the early stages of pregnancy.
Why TSH “Normal” Is Not Enough?
In the world of IVF and RIF, "normal" is not good enough; we aim for "optimum." While a TSH up to 4.0–4.5 mIU/L may be acceptable for general health, it is often too high for a successful embryo transfer.
- The Target: We typically aim to keep the TSH below 2.5 mIU/L before and during the early stages of the embryo transfer cycle.
- The "Switch": Think of the thyroid as the master metabolic switch. If it is sluggish (hypothyroidism), the uterine lining may not receive the metabolic signals required to become fully receptive to the embryo.
Dr. Jay Mehta’s Advice: Thyroid dysfunction is arguably the most easily correctable factor in our RIF practice.
It simply requires a small daily tablet and a blood test every few weeks. Never skip this evaluation; it’s a simple fix that can prevent years of heartbreak.
Why Thyroid Health is Often Missed?
Because thyroid symptoms (fatigue, weight gain, or feeling cold) are often subtle, they are frequently dismissed. However, in the context of RIF, we must be aggressive in our screening:
- Comprehensive Screening: We test for TSH, Free T3, Free T4, and Anti-TPO antibodies as a standard part of the RIF panel.
- Pre-Transfer Optimization: We ensure your thyroid levels have been stable in the optimum range for at least 4 to 6 weeks before we proceed with an embryo transfer.
Practical Next Steps for Your Journey
If you suspect thyroid issues or have had multiple failed transfers, take these steps:
- Get the Titer: Ask your doctor specifically for an Anti-TPO Antibody test, not just a basic TSH screen.
- Check the Timing: Thyroid medication (Levothyroxine) should be taken on an empty stomach, at least 30-60 minutes before breakfast, to ensure proper absorption.
- Monitor Frequently: Once you conceive, thyroid requirements can increase by 30-50% almost immediately. Ensure you have a plan for rapid testing once you get a positive result.
As a specialist in complex RIF, I look for every "easy win." Optimizing your thyroid is a simple, low-cost, and highly effective way to remove a major barrier to your success.
Is your thyroid health being overlooked in your current treatment plan? Let’s conduct a comprehensive thyroid and antibody review to ensure your "master switch" is set for success. Consult with Dr. Jay Mehta at Shree IVF Clinic for a specialized thyroid & RIF evaluation.
Is Obesity the Hidden Metabolic Barrier Behind Your Implantation Failure?
Obesity is the single most significant detrimental factor in achieving a successful embryo implantation.
It creates a state of chronic hormonal imbalance that damages the window of implantation (WOI) and degrades both egg and sperm quality.
Achieving a BMI closer to 26, or losing 10-15% of total body weight, is often the most effective "medicine" for recurrent failure.
How Obesity Shifts the Window of Implantation?
When a patient’s BMI exceeds 30, the body enters a state of metabolic inflammation. This doesn't just affect general health; it fundamentally alters the uterine lining.
- Altered Hormones: Excess fat tissue acts like an endocrine organ, converting hormones into estrogen. This "extra" estrogen confuses the signals sent to the uterus.
- Displaced WOI: This hormonal noise causes a massive shift in the Window of Implantation. The embryo may arrive on time, but the uterus is either "closed" or "out of sync" due to the metabolic environment.
Modern Solutions: From "GLP-1" Drugs to Bariatric Surgery
At Shree IVF Clinic, we don't just tell patients to "eat less." We use a multidisciplinary approach involving bariatric surgeons and endocrinologists to manage weight effectively.
- Revolutionary Medications: Drugs like Ozempic and Mounjaro have transformed weight loss. We use these to stabilize the patient over a prolonged period.
- The Safety Rule: We must stop these medications at least three months before an embryo transfer to ensure a safe pregnancy environment.
- Bariatric Surgery: For severe cases, surgery is a powerful tool to reset the body's metabolism.
- The Waiting Period: After bariatric surgery, the body undergoes intense nutritional changes. The patient must wait at least one year before undergoing an embryo transfer.
Dr. Jay Mehta’s Advice: We aim for a 'reset.' Dropping 10-15% of your weight or reaching a BMI of 26 can do more for your success rates than any expensive immunotherapy. It brings the implantation window back to its natural timing.
The "Silent" Male Factor in Obesity
We must not overlook the male partner. Obese males face a unique and sometimes permanent challenge:
- Estrogen Conversion: In obese males, fat tissue converts testosterone into estrogen. This chronic exposure to high estrogen levels can cause severe, sometimes irreversible damage to the seminiferous tubules where sperm are developed.
- Sperm Quality: This leads to poor sperm quality and, in some cases, azoospermia (zero sperm count). While weight loss helps, the damage from long-term obesity can be difficult to fully reverse.
Practical Next Steps for Your Journey
If obesity is a factor in your recurrent failures, follow this clinical roadmap:
1. Multidisciplinary Consultation: Don't just see a fertility doctor. Get a joint evaluation with an endocrinologist to check for insulin resistance and metabolic markers.
2. Targeted Weight Loss: Aim for the 10-15% milestone. This isn't about "looks"; it's about shifting your internal chemistry to be receptive to a pregnancy.
3. The Wait-and-Prep Period: If you choose bariatric surgery or GLP-1 drugs, respect the waiting periods (1 year for surgery, 3 months for drugs). This is vital for the safety of your future baby.
As a specialist in RIF, I view weight management as an essential part of the IVF protocol, not an "extra." It is one of the most treatable lifestyle changes.
By correcting the BMI, we aren't just helping you get pregnant; we are ensuring a safer, healthier pregnancy for both you and your child.
Low Progesterone and Implantation Failure: Facts vs. Myths
While progesterone is the hormone of pregnancy, "low progesterone" is rarely the true cause of failure in a medicated IVF cycle because external support is always provided.
While we aim for a progesterone level between 10 and 80 ng/mL during the transfer window, routine progesterone testing is not always necessary for a successful outcome.
The Reality of Progesterone Testing in IVF
At Shree IVF Clinic, we do not routinely test serum progesterone levels during an IVF cycle or even on the day of the embryo transfer. Here is the clinical reasoning:
- External Support: In almost every IVF cycle, patients are given high doses of external progesterone (via injections, gels, or tablets). This ensures the body has more than enough of the hormone to support implantation.
- The Normal Range: If a test is performed, a value between 10 and 80 ng/mL is considered healthy for an embryo transfer window.
- Natural vs. IVF Cycles: In a natural conception, a progesterone level of 25 ng/mL or more is ideal at the time of implantation. However, in IVF, the external medication overrides the body's natural production, making "low levels" virtually impossible if the medication is taken correctly.
Understanding Luteal Phase Defect (LPD)
In patients who conceive naturally, a condition called Luteal Phase Defect can occur.
This is when the ovary does not produce enough progesterone to maintain the uterine lining, potentially leading to recurrent early abortions.
- The Simple Fix: This is easily corrected by administering external progesterone support during the luteal phase (the second half of the menstrual cycle).
- The IVF Advantage: Because IVF protocols already include this "support" as a standard step, the risk of a luteal phase defect causing failure is essentially eliminated.
Does a Slightly “Low” Value Mean Failure?
Many patients worry that a "low" number on a blood test means their transfer will fail. However:
- No Concrete Evidence: There is no documented scientific study proving that a slightly lower progesterone level has a severe negative impact on implantation, provided the patient is on a standard replacement protocol.
- Absorption Variability: Blood tests don't always reflect the concentration of progesterone directly inside the uterine tissue, which is where it matters most.
Practical Next Steps for Your Journey
If you are concerned about your progesterone levels, follow these practical guidelines:
- Consistency is Key: The most important factor isn't the blood level but the timing and consistency of your progesterone medication. Never miss a dose.
- Trust the Protocol: If you are on a medicated (frozen) embryo transfer cycle, your doctor has already accounted for your body's needs by providing external support.
- Natural Cycle Support: If you are trying naturally and have had early losses, discuss "Luteal Phase Support" with your doctor to see if supplemental progesterone is right for you.
In my practice, I focus on the factors that truly move the needle—like embryo quality and the uterine environment.
While progesterone is vital, we treat it as a foundational part of the protocol rather than a variable we need to obsessively monitor.
Are you worried about your hormone levels for your upcoming transfer? Let’s focus on a robust support protocol that ensures your uterus is perfectly prepared for your embryo.
Does Vitamin D Really Improve Implantation in IVF?
Vitamin D is no longer just a "vitamin"—it acts as a pro-hormone that is essential for the uterine lining to "accept" an embryo. Vitamin D levels are associated with better implantation and pregnancy outcomes
Because chronically low levels are proven to negatively affect implantation, vitamin D supplementation has become a global standard of care, often given to every IVF patient without the need for expensive repeated testing.
Why is Vitamin D Essential for the Uterus?
Scientific research has shown without a doubt that Vitamin D plays a critical role in the "dialogue" between the embryo and the mother. It isn't just about bone health; it is about endometrial receptivity.
- The "Welcome" Signal: Vitamin D helps the endometrium (uterine lining) transform into a receptive state. Without adequate levels, the lining may not respond correctly to the signals sent by the embryo.
- Immune Modulation: It helps regulate the local immune environment in the uterus, preventing the mother’s body from seeing the embryo as a "foreign object" and rejecting it.
- The Chronic Deficiency Risk: Patients with extremely low or chronically deficient Vitamin D levels consistently show lower implantation rates compared to those with optimal levels.
Why Many IVF Clinics Supplement Without Repeated Testing?
At Shree IVF Clinic, and in most leading fertility centers worldwide, we treat Vitamin D as an empirical therapy.
- No Testing Burden: Instead of making every patient undergo repeated blood tests to check their Vitamin D levels—which can fluctuate and add to the cost—we provide supplementation to everyone.
- Safety and Standardization: Because the safety profile of Vitamin D is excellent and the benefits for implantation are so high, it is more efficient to ensure every patient reaches an optimal level through standardized oral or injectable doses before the transfer.
How Does Vitamin D Affect the IVF Outcome?
When your Vitamin D levels are corrected, we see a tangible improvement in the "response" of the system:
1. Improved Lining Quality: The endometrium often appears more robust and ready for the transfer.
2. Higher Clinical Pregnancy Rates: Studies suggest that women with sufficient vitamin D levels have a significantly higher chance of a successful live birth following embryo transfer.
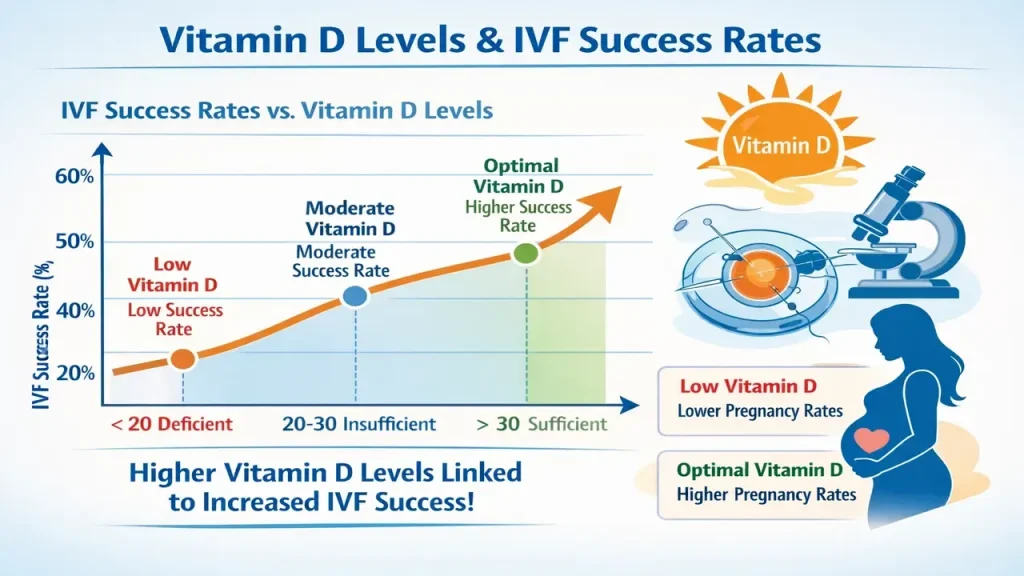
Dr. Jay Mehta’s Advice: In the world of RIF, we look for every possible advantage. Vitamin D is a simple, cost-effective, and powerful tool.
We don't wait for a deficiency to show up on a test; we supplement it to ensure your 'soil' is as fertile as possible for the 'seed.'
Next Steps for Your Journey
If you are preparing for an embryo transfer, follow these simple vitamin D guidelines:
- Start Early: Begin supplementation at least 4 to 8 weeks before your planned transfer to allow levels to stabilize in your tissues.
- Follow the Protocol: Whether it is a weekly sachet or a daily tablet, stay consistent. Vitamin D is fat-soluble and builds up over time.
- Don't Stress the Test: If your clinic has already started you on a supplement, don't worry about testing your levels independently. Trust that the standardized dose is designed to put you in the "success zone."
Is There a Cure for Recurrent Implantation Failure (RIF)?
There is no single "magic pill" or cure for RIF because it is not a single disease—it is a result of various underlying factors.
However, through a systematic diagnostic protocol, we can identify the cause in approximately 60% of cases.
For the remaining 40% where a diagnosis remains elusive, success depends on the clinical experience of the specialist and the use of targeted, evidence-based reserve therapies.
The 60/40 Diagnostic Reality
In our specialized RIF unit, we find that patients generally fall into two categories:
- The Explained 60%: In the majority of cases, we find a concrete reason for failure. Whether it is a structural issue (like a fibroid or endometriosis) or a specialized metabolic problem, these have a high "cure" rate. Once the pathology is surgically or medically corrected, the patient often conceives in the very next cycle.
- The Unexplained 40%: These are the most challenging cases where all tests come back normal. Here, we rely on empirical and reserve therapies based on years of clinical experience to tilt the odds in the patient's favor.
Correctable Causes: The "Easy Wins"
Many patients suffer through multiple failed cycles simply because a structural or medical issue was overlooked. Once identified, these are highly treatable:
- Surgical Correction: Conditions like Fibroids, Endometriosis, or Adenomyosis can be definitively treated by a dedicated surgical team. Removing these barriers often "cures" the RIF immediately.
- Immunological Management: If a patient has a diagnosed immunological disease, we collaborate with a rheumatologist. By giving the correct immunosuppressant medication, we can neutralize the body's overactive defense system and allow implantation to occur.
The Role of Reserve Therapies (For Unexplained RIF)
For the "unexplained" 40%, we utilize powerful reserve protocols. These are not "random" treatments but calculated interventions:
- Reserve Protocols: We use specific combinations of drugs like Thymosin Alpha and Tacrolimus. These are potent immune modulators that must be dosed with extreme precision.
- Safety First: Because these are immunosuppressants, we prioritize patient safety. In our clinic, we seek advice from a nephrologist before administering these drugs, as they are experts in how these medications affect renal (kidney) tissue.
Why You Need a Dedicated RIF Specialist?
If you have experienced two or more failed IVF cycles, you should not simply repeat the same treatment. A dedicated RIF clinic provides:
- Diagnostic Protocol-Based Evaluation: Moving away from "blind" treatments.
- Multidisciplinary Expertise: Access to surgeons, rheumatologists, and nephrologists to handle complex cases.
- Experience-Led Empirical Care: For unexplained cases, the intuition and experience of a specialist are your greatest assets.
Dr. Jay Mehta’s Advice: "Don't settle for 'unexplained' until every stone has been turned.
Most RIF is not a permanent state; it is a hurdle that can be cleared with the right diagnosis and a specialized team."
Final Takeaway
Is there a cure for RIF? Not a single pill. Not a universal protocol.
But in many cases—yes, there is a solution. With proper diagnosis, surgical precision (when needed), targeted medical therapy, and experienced specialist care.
Recurrent implantation failure can often be overcome.
Why Protocol Changes Alone Don’t Solve Recurrent Implantation Failure (RIF)?
Changing an IVF stimulation protocol helps with embryo quantity and "standard" failures, but it rarely solves Recurrent Implantation Failure (RIF).
In RIF, the problem is often not the "making" of the embryo—many patients already have genetically normal, high-grade embryos—but the "interaction" between that embryo and the uterus.
If the foundation is broken, changing the way you stimulate the ovaries won't fix the result.
The "Good Embryo" Paradox
A common misconception is that if an IVF cycle fails, the "stimulation" was wrong. However, for patients referred to a dedicated RIF clinic, the reality is often different:
- High-Grade Embryos: Many RIF patients are excellent "embryo makers." They often have multiple Grade-A blastocysts.
- Genetically Normal (PGT-A): A large percentage of RIF patients have already used PGT-A to confirm their embryos are chromosomally normal.
In these cases, the IVF protocol (the way the eggs were collected) was actually successful. Changing it further is unlikely to be the "cure" because the failure is happening after the embryo is created.
Stimulation vs. Implantation: Two Different Stages
It is vital to distinguish between the two different stages of the process:
| Stage | Focus | When it’s the Problem |
|---|---|---|
| Ovarian Stimulation | Changing drugs to get more/better eggs | Low egg reserve or poor fertilization |
| Implantation | Fixing the uterus, metabolism, or immune system | Recurrent Implantation Failure (RIF) |
When Do We Actually Change the Stimulation Protocol?
We only change the IVF stimulation protocol if there is a very specific, data-driven requirement, such as:
- Evidence of Paternal Stress: If embryos are fragmented early in previous cycles, indicating a need for different sperm selection or antioxidant protocols.
- Persistent Poor Egg Quality: If the embryos were consistently low-grade, despite the male factor being normal.
- Paternal Stress Indicators: If early embryo fragmentation suggests oxidative stress or sperm-related factors.
- PCOS-Related Issues: If the previous protocol led to severe OHSS or poorly matured eggs.
Dr. Jay Mehta’s Advice: If you have already created genetically normal embryos and they didn't stick, the answer isn't in a different injection for your ovaries.
The answer is in the 'detective work' inside the uterus and your body’s metabolic environment. We don't change what is already working; we fix what is failing.
The RIF Strategy: Investigation Over Iteration
Instead of blindly changing the protocol, we focus on:
1. Structural Audit: Is there a hidden fibroid or endometriosis?
2. Lining Integrity: Is there chronic inflammation (endometritis)?
3. Metabolic Sync: Is your thyroid or insulin resistance sabotaging the window of implantation?
Our goal at Shree IVF Clinic is to stop the cycle of "trying again" with just a different brand of medication. We move the focus away from the ovaries and onto the implantation site.
Success in RIF comes from diagnosing the reason for the failure, not just iterating the stimulation.
Have you been told to just "try another protocol" after multiple failures? Let’s look beyond the stimulation and find the real reason your embryos aren't sticking. Consult with Dr. Jay Mehta for a Truthful RIF Evaluation and Targeted Treatment Plan
Why Is a “Freeze-All” Strategy Preferred in Recurrent Implantation Failure (RIF)?
For patients fighting recurrent implantation failure (RIF), a "Freeze-All" strategy is almost non-negotiable.
By freezing all embryos, we bypass the hormonal chaos of the stimulation phase, allow the uterus to return to its natural state, and provide the necessary time for advanced genetic testing (PGT-A).
1. Bypassing the "Hormonal Storm"
During an IVF stimulation cycle, your hormone levels (specifically estrogen and progesterone) reach levels much higher than in a natural cycle.
- The Problem: These high hormones can make the uterine lining "mature" too quickly, causing a mismatch between the embryo and the uterus.
- The Solution: In a Freeze-All cycle, we collect the eggs and create embryos, but we do not transfer them immediately. We wait for your hormones to return to baseline, ensuring that when we do the transfer later, the "soil" is perfectly calm and receptive.
2. The Necessity of Genetic Testing (PGT-A)
As we have discussed, a critical pillar of treating RIF is ensuring the embryo is genetically normal.
- The Logistics: PGT-A requires a small biopsy from the blastocyst. These cells are sent to a specialized lab for analysis, a process that typically takes 10–14 days.
- Mandatory Freezing: Because we cannot keep a blastocyst in the incubator for 14 days, the embryos must be frozen immediately after the biopsy. Without a "freeze-all" approach, precision genetic screening is impossible.
3. Optimizing the Implantation Window
A fresh transfer forces you into a "one-size-fits-all" timeline. A Frozen Embryo Transfer (FET) allows us to:
- Customize the Timing: We can precisely control exactly how many hours of progesterone your lining needs before the transfer.
- Perform "Silent" Healing: The gap between the "Freeze" and the "Transfer" gives us time to treat issues like chronic endometritis or thin lining without being rushed by a growing embryo.
4. Reducing the Risk of OHSS
For many RIF patients—especially those with PCOS—the high egg counts required for success increase the risk of Ovarian Hyperstimulation Syndrome (OHSS).
A Freeze-All strategy essentially eliminates the risk of severe OHSS, making the entire journey much safer for the patient.
Dr. Jay Mehta’s Advice: In RIF, we don't want to rush. A fresh transfer is like trying to plant a seed during a hurricane. We freeze all embryos to wait for the storm to pass, test the seeds for quality, and then plant them when the soil is perfectly prepared.
If you are starting a new IVF cycle after previous failures, ensure your plan includes:
1. A "Freeze-All" Intent: Discuss with your doctor that you do not want a fresh transfer, regardless of how the lining looks on the day of trigger.
2. Biopsy Coordination: Ensure the lab is equipped for trophectoderm (blastocyst) biopsy and vitrification (ultra-fast freezing).
3. Preparation Month: Use the month after the freeze-all to perform any final uterine checks (like a hysteroscopy or MUM-1 test) before the actual transfer.
At Shree IVF Clinic, the freeze-all strategy is a cornerstone of our success in complex RIF cases.
It gives us the control we need to ensure that when we finally perform your transfer, every variable—from the embryo’s genetics to the uterine receptivity—is in your favor.
Are you being pushed toward a fresh transfer despite previous failures? Let’s talk about why a freeze-all strategy might be the safer, more successful path for you.
The Emotional Impact of RIF: Navigating the Trauma of "Not Knowing"
Recurrent implantation failure is more than a medical challenge; it is a state of deep emotional, physical, and mental exhaustion.
By the time patients reach an RIF clinic, they have often endured years of trauma.
Navigating this requires radical honesty from the medical team, realistic expectations, and a strong support system rather than "false promises."
The Reality of "Total Exhaustion"
Patients who arrive at a specialized RIF unit are rarely at the beginning of their journey. They are usually at their breaking point.
- The Physical Toll: Years of injections, hormonal fluctuations, and surgical procedures.
- The Financial Toll: The heavy burden of multiple IVF cycles without a result.
- The Emotional Toll: The repeated cycle of hope during a transfer followed by the crushing grief of a negative result.
At Shree IVF Clinic, we recognize that we are not just treating a uterus or an embryo; we are treating a human being who is hurting.
Honesty Is Not Harsh — It Is Compassion
In a country like India, patients are often given "fake promises" or told to just "try one more time" without a change in strategy. We believe this is a disservice to the patient.
- Radical Candor: We are known for being brutally honest. If the situation is difficult or the prognosis is guarded, we tell you.
- Realistic Expectations: We don't sell "miracles"; we provide data-driven strategies. In the long term, patients appreciate knowing the truth because it allows them to make informed decisions about their lives and their families.
- Counseling Support: Professional counseling is a vital part of the RIF journey to help manage the trauma of repeated failures.
The Vital Role of Family Support
In the Indian social context, the pressure to conceive can be immense.
- The Shared Burden: The family must understand that RIF is a medical condition—often involving complex factors like genetics or paternal epigenetics—and not a "failure" of the woman.
- A Shield for the Patient: A supportive family acts as a buffer against social pressure, allowing the couple to focus on the specialized diagnostic evaluations needed to move forward.
Dr. Jay Mehta’s Advice: My job is to be your doctor, not your cheerleader. I will give you the truth, however difficult it may be. Compassion in RIF isn't about giving you a false 'yes'; it's about standing by you with a scientific plan and a realistic perspective so you can find a way out of the trauma.
The Path to Emotional Healing
If you are currently feeling overwhelmed by previous failures, remember:
1. It is okay to grieve: Each failed transfer is a loss. Permit yourself to feel that before jumping into the next cycle.
2. Seek a Specialist: Much of the trauma of RIF comes from the "unknown." A specialist who gives you a diagnosis can often provide the emotional relief of finally having an answer.
3. Prioritize Your Relationship: Don't let the pursuit of a baby destroy the bond with your partner. Take breaks when needed.
As a specialist, I see the strength it takes to keep going after multiple failures. We respect that strength by providing a clinic environment that is considerate, honest, and scientifically rigorous.
You are not a number; you are a patient who deserves the truth and a path forward.
Are you feeling emotionally exhausted by unexplained failures? Let’s sit down for an honest discussion about your situation and create a plan based on reality, not just hope.
How Do You Cope with Repeated IVF Failure?
You cope by not carrying it alone—medically or emotionally.
Coping with Recurrent Implantation Failure (RIF) requires more than medical intervention; it requires a reservoir of mental, emotional, and financial resilience.
While the medical team provides the clinical roadmap, the weight of the journey is often best shared with those who have walked the same path.
We believe that dedicated support groups—led by patients for patients—are the key to navigating this marathon.
The Unique Burden of Repeated Failure
Repeated failure is a unique kind of grief. Unlike a sudden loss, it is a "rolling" trauma that repeats with every negative pregnancy test.
- The Clinical Friendship: Because the RIF journey is long and complex, our patients often become more than just numbers—they become friends. We see firsthand the incredible strength they muster to keep going.
- Decision Fatigue: After multiple failures, making medical decisions becomes exhausting. This is where the clarity of a specialized medical team is vital to prevent "random" treatment choices driven by desperation.
The Power of the Support Group
We strongly advocate for the creation of patient-led support groups. At Shree IVF Clinic, we encourage our successful "graduate" patients to guide those still in the struggle.
- Peer Guidance: Talking to someone who has faced the same 2–3 failed transfers and eventually found success provides a level of hope that no doctor can offer.
- Emotional Safety: A support group provides a space where you don't have to explain your pain; everyone in the room already understands it.
- Concrete Decisions: Hearing how others navigated the choice between further testing, donor eggs, or specialized surgeries can help you take more confident steps in your own treatment.
The Balance: Emotional Support vs. Clinical Judgment
While support groups are essential for emotional survival, the "medical rudder" must remain in the hands of the specialist.
- Avoiding Misinformation: Every RIF case is different. What worked for a friend in a support group (like a specific blood thinner or immune drug) may not be right for your body.
- Sound Clinical Judgment: All final medical decisions must be based on your diagnostic data—your hysteroscopy results, your embryo's PGT-A report, and your metabolic markers.
Dr. Jay Mehta’s Advice: "I pray for my patients to stay strong, but I also know that even the strongest steel can bend. Don't carry this alone. Use a support group for your heart, but use your medical team for your head. Together, we find the path to success."
Practical Ways to Cope Right Now
If you are struggling with a recent failure:
1. Join (or Start) a Support Circle: Seek out communities of RIF survivors who prioritize science and emotional health over myths.
2. Financial Planning: RIF is expensive. Sit down with your team to discuss a long-term financial strategy so that money doesn't become a sudden barrier to the "final" successful transfer.
3. Trust the Detective Work: Remember that each failure, while painful, provides data. Use that data to refine the plan rather than just repeating the same mistakes.
We don't just want to help you get pregnant; we want you to reach the finish line with your mental health intact.
Our clinic is committed to being a transparent, honest partner in your journey, providing the clinical expertise you need while encouraging the emotional support you deserve.
Are you feeling isolated by your journey? Let’s connect you with the right resources and a medical plan that prioritizes your well-being as much as your success.
Why Are Anxiety and Depression So Common in RIF Patients?
Because Recurrent Implantation Failure (RIF) carries an invisible emotional weight—the loss of control.
Even when everything looks “perfect” medically—a genetically tested embryo, a corrected uterus, optimized hormones—implantation may still not occur. That unpredictability is what drives deep anxiety and, over time, depression.
We manage this heavy emotional burden through radical honesty, realistic goal-setting, and clear written documentation to provide certainty in an uncertain journey.
The Psychology of the "Final Say"
In most areas of life, hard work and expert help lead to a predictable result. In RIF, this isn't always the case.
- The Nature Variable: You can have a perfect, genetically tested embryo and a surgically corrected uterus, yet implantation may still not occur. This lack of control is the primary driver of anxiety.
- The Dream vs. Reality: When outcomes don't match the dreams a couple has held for years, depression often sets in. It is a natural response to a prolonged, high-stakes struggle.
Honesty as an Antidote to Anxiety
At Shree IVF Clinic, we have found that "toxic positivity" (giving false hope) actually increases anxiety.
- The Value of Realistic Counseling: We provide honest, data-driven counseling. While the truth may feel difficult to hear initially, it provides a stable foundation.
- Long-term Relief: Patients eventually realize that knowing the true odds and the specific challenges allows them to prepare mentally, rather than being constantly blindsided by failure.
The Role of Written Documentation
Anxiety often stems from the "fog" of a consultation—forgetting what was said or doubting the plan. In India, where family involvement and social pressure are high, this is especially common.
- Clarity in Writing: We provide our patients with written documentation of their diagnosis, the proposed plan, and the realistic success rates.
- A Tool for Doubt: Whenever anxiety spikes or a family member asks a question, the patient can refer back to the written document. This "hard evidence" acts as an emotional anchor, significantly reducing treatment-related stress.
Coping Strategies for the RIF Journey
If you are currently struggling with the emotional weight of RIF, we recommend these steps:
1. Acknowledge the Trauma: Recognize that what you are feeling is a normal reaction to an abnormal amount of stress.
2. Information Control: Rely on the written plan provided by your specialist rather than searching the internet, which often fuels anxiety with misinformation.
3. The "Truth" Over "Promises": Choose a medical team that values honesty. A doctor who tells you the risks is often more trustworthy than one who only gives you "fun promises."
My role is to be your clinical guide and your source of truth. We don't just want to help you conceive; we want you to navigate this process without losing your mental well-being.
By combining honest communication with clear documentation, we aim to strip away the "fear of the unknown" that fuels anxiety and depression.
Are you feeling overwhelmed by the uncertainty of your next steps? Let’s sit down, look at the data, and give you a written plan that brings clarity back to your journey. Consult with Dr. Jay Mehta at Shree IVF Clinic for an Honest & Documented RIF Strategy
Why Is Psychological Support Essential in Recurrent Implantation Failure (RIF)?
At a specialized RIF clinic, psychological support is not an "optional extra"—it is a core medical requirement.
Patients often arrive with significant emotional trauma, and the courage it takes to start "one more time" is immense.
We provide this support through dedicated professional counselors and a scientifically informed team to ensure your hope is grounded in reality.
1. The "Courage to Restart."
Most patients seeking help for recurrent implantation failure have already faced the crushing blow of a negative result multiple times.
- The Trauma of Failure: The psychological weight of previous failures can lead to a state of "learned helplessness."
- Building Resilience: Our team is specifically trained to recognize the signs of emotional exhaustion. We work to rebuild the patient's confidence, not through empty encouragement, but by acknowledging the trauma they have already endured.
2. Integrated Counseling Support
At Shree IVF Clinic, psychological care is woven into the medical protocol:
- Dedicated Counselors: We have professional counselors available to help patients navigate the complex feelings of grief, anxiety, and the high-stakes pressure of a new cycle.
- Trained Team Members: From the nursing staff to the senior doctors, our entire team is trained in psychological support. We understand that every interaction—whether it’s a blood test or a scan—is an emotional event for an RIF patient.
3. Science as an Emotional Anchor
Interestingly, one of the best forms of psychological support is clear, scientific information.
- Reducing the Unknown: Anxiety thrives in uncertainty. By explaining the "why" behind a failure and the "how" of the new plan, we replace fear with understanding.
- Realistic Expectations: We are careful never to provide "false hope." Giving a patient a realistic percentage of success and a clear scientific roadmap helps them manage their emotional investment. When you know exactly what to expect, the "shocks" of the journey are significantly minimized.
4. Supporting the "Hope" Molecule
We recognize that when a patient starts a new treatment at our unit, they are bringing their last bit of hope. Our role is to protect that hope by:
- Honest Fact-Sharing: Ensuring the patient understands the probable outcomes.
- Consistent Availability: Being there to answer the "what ifs" that keep patients awake at night.
- Validation: Simply acknowledging that "it is okay to be scared" can be incredibly healing.
Dr. Jay Mehta’s Advice: "My team and I are here to hold the scientific side of the equation so that you can focus on the emotional side.
We don't expect you to be 'brave' every day; we expect you to be human. Let our counseling team support your mind while we support your body."
Practical Next Steps for Emotional Support
If you are preparing to start another cycle after RIF, consider these steps:
1. Schedule a Pre-Treatment Counseling Session: Don't wait for a crisis; speak to our counselor before the cycle begins to build a "mental toolkit."
2. Ask for the Data: If you feel anxious about a procedure, ask for the scientific facts. Clarity is the enemy of anxiety.
3. Involve Your Partner: Ensure both partners are involved in the counseling process, as the emotional burden is shared.
We see the person, not just the diagnosis. By combining advanced embryology with compassionate psychological support, we aim to make your journey as smooth as possible, regardless of how difficult the previous path has been.
Would you like to speak with our dedicated counselor to help prepare your mind and heart for your next treatment steps? Call 1800-268-4000
Can You Still Have Hope After Recurrent Implantation Failure (RIF)?
Hope in the context of Recurrent Implantation Failure (RIF) should not be based on blind faith or "good luck."
Instead, it should be grounded in the fact that RIF is a rapidly emerging science. When you shift your journey from a standard clinic to a specialized RIF unit, your hope is rebuilt on a foundation of clinical expertise, individual diagnostics, and data-driven guidance.
1. Moving Beyond "Hope-Based" Treatment
In standard IVF, patients often "hope" that this cycle will be the lucky one. In RIF, "hoping for luck" is what leads to emotional trauma.
- The Emerging Science: We now have tools to look at the genetics of the embryo, the microbiome of the uterus, and the metabolic health of the mother.
- The Scientific Shift: When we find a specific reason for a failure—such as chronic inflammation or a displaced implantation window—the "hope" becomes a strategy.
2. Trusting the Specialist’s Expertise
The most effective way to reduce the mental trauma of RIF is to delegate the clinical burden to an expert.
- Expert Guidance: Once you have chosen a specialist, your role is to focus on your emotional well-being while the medical team focuses on the "detective work."
- Individualized approach: A specialist does not offer a "menu" of treatments. They provide a specific, case-based path that is of the most benefit to your unique situation.
3. Replacing Uncertainty with a Plan
The "trauma" of RIF usually stems from the feeling of being lost. A specialized RIF clinic replaces that void with a concrete diagnostic protocol:
- Investigation: Finding the "Why" through advanced testing.
- Correction: Fixing the "why" through surgery or medication.
- Execution: Performing the transfer only when all variables are optimized.
Dr. Jay Mehta’s Advice: "I tell my patients, 'Give me your medical history, and let me carry the weight of the science.
You have already done the hard work of building the courage to try again. Now, let the emerging science of RIF provide the roadmap to your success."
4. Realistic Hope is the Best Hope
True hope comes from knowing that you aren't just repeating the same mistakes. It comes from:
- A Clear Diagnosis: Finally knowing why previous cycles failed.
- Precision Medicine: Using drugs like Tacrolimus or LMWH only when specifically needed.
- Genetic Certainty: Knowing your embryo is chromosomally normal (PGT-A).
At Shree IVF Clinic, we believe that the best way to support a patient is to be an expert navigator.
We don't want you to "wish" for a baby; we want to build the medical circumstances that make that baby a reality.
By leaving the medical complexities to us, you can find the mental peace needed to finish this journey.
Are you ready to stop "hoping" and start "investigating"? Let’s look at the science behind your failures and build a plan that gives you a genuine reason to be optimistic.
Consult with Dr. Jay Mehta at Shree IVF Clinic to turn your RIF journey into a success story.

Dr. Jay Mehta
MBBS, DNB—Obstetrics & Gynecology
IVF & Endometriosis Specialist, Laparoscopic Surgeon (Obs & Gyn)

4.9
![]()
Verified & Most Trusted One
Dr. Jay Mehta is a highly renowned IVF specialist and fertility-preserving surgeon based in Mumbai, India. As the director of the Shree IVF and Endometriosis Clinic, Mumbai, he is recognized as one of India's leading laparoscopic gynecologists for the advanced treatment of complex conditions such as endometriosis and adenomyosis.
Dr. Mehta's expertise extends deeply into reproductive medicine; he is a well-known IVF specialist and among the few practitioners in the country with specialized knowledge in embryology, andrology, reproductive immunology, and Mullerian anomalies. Dr. Mehta conducts operations and consultations across India's major cities, including Pune, Chennai, Hyderabad, Bangalore, Ahmedabad, Agra, and Delhi. To book an appointment, call: 1800-268-4000
Many Treatments. One Goal.
Caring for Every Patient, Every Day.
ALPA AINCHWAR
Thank you to the best endometriosis surgeon in our India.
Honest and very ethical person.
I want to add one thing, very respectful behavior towards all the patients here.
The only thing is doctor jay is very straight forward.
If he is getting so much work being so straight forward. I can only imagine what will happen if he becomes little sweet and sugary sugary to everyone. But whatever I know him he won’t become like that, kyunki iss Bande ko bhagwaan ka kuch alag aashirvaad hai
Vidhi Mehta
Dr Jay Mehta is a genius at treating endometriosis patients. To the point, no bakwaas. For 13 years I was made to believe I could never conceive naturally, from the age of 19 when I went to a hospital for the first time as an emergency endo patient.
After 2 endo surgeries, 1 failed IVF and a miscarriage here I meet the first doctor who said you will conceive naturally. (Hope). , This was God’s plan, Lord Shiva!!
Thank you Dr. Jay, Dr. Vismay, and the entire team for the hope, treatment, hospitality, and the quickest discharge.
RENUKA RAUT
Great Experience. I have been operated for grade 4 endometriosis. I have never seen a doctor like Jay Sir in my entire life..he is very concerned about his patients..going out of the way to make things possible
Finally, I found an endometriosis specialist after struggling a lot. I am In a safe hand. Each and every staff of this hospital is well-trained and well-managed..highly recommended
Sunitha Suni
He is the god me because im suffering from since 4year pain full period of endometriosis problem im going to so many hospitals any one not identify the problem he is identify and clear endometriosis problem, thanq Dr jay metha sir, Dr Chaitali Rao and ur team Good receiving thanq so much sir ur save my life
md Sohail
Dr. Jay Mehta, what a doctor he is ..hats off.
I really wanted to thank from the bottom of my heart to Dr. Jay Mehta and his dedicated and caring team.
We came from Hyderabad and undergone a major surgery. What a guts he has. I highly recommend Dr Jay Mehta for women who needs a cure for Endometriosis.
Huge thanks to Dr. Chaitali, Dr. Vismai sir and all the supporting staff, nurses and mausis. He is the great doctor and do the best treatment.
Overall very rare kind of personality is Dr.Jay Mehta among the present generation of doctors.
Ankit Jain
I wanted to thank Dr. Jay and his dedicated and caring team at Shree IVF & Endometriosis Hospital at Ghatkopar, Mumbai for the Endometriosis surgery performed. His knowledge of this dreadful disease and its treatment to help thousands of endometriotic women is truly amazing.
He is a gem of a person, explains the problem to patients and their families nicely, and proposes surgical treatment. His caring team also makes the stay in the hospital post-op help to recover quickly.
I highly recommend Dr Jay Mehta for women who need a cure for Endometriosis. He also works brilliantly for IVF and other gynac issues. Kindly check with the clinic and hospital and plan your visit accordingly. They also help with nearby stays for outstation patients. God bless you and give you the strength to continue to work in the noble field.
Blogs
How to Avoid Pregnancy Naturally After Sex?
Learn what emergency contraception works, when to take it, & which natural methods actually prevent pregnancy

2-Hour Urine Hold Pregnancy Test Explained: A Simple Guide
The 2-hour urine hold method helps ensure accurate pregnancy results by increasing hCG concentration, allowing for early detection even before you missed period
Videos
Importance of the Fallopian Tubes in Fertility
Fallopian tubes play a key role in fertilization by transporting the egg and sperm. Blocked or damaged tubes can prevent natural pregnancy

Best Sex Position to Get Pregnant Naturally
Best positions to get pregnant—try missionary or using pillows under your hips. Small changes can boost your chances of conceiving