Home » Gynaecology » Uterine fibroids (leiomyomas): Symptoms, Causes, Types, Diagnosis & Treatment
Uterine Fibroid Treatment in Mumbai – Advanced Fertility & Uterus-Preserving Care

Yes, fibroids can certainly be treated effectively, and in most cases, we can do so while preserving your fertility.
At Shree IVF Clinic, I, Dr. Jay Mehta, believe in empowering my patients with clear, accurate information so you feel confident about every step of your care.
Uterine fibroids are non-cancerous growths that commonly develop in the uterus and can vary in size, location, and impact. While the presence of fibroids may sound alarming, I want to reassure you that these are manageable with the proper care tailored to your unique circumstances.
We provide world-class, fertility-preserving uterine fibroid treatment here in Mumbai, India.
Whether you are struggling with painful symptoms like heavy menstrual bleeding or pelvic pain or facing challenges with conception, we are here to provide you with transparent guidance, advanced surgical expertise, and unwavering support on your journey back to health.
What Are Uterine Fibroids?
It is important to understand that a uterine fibroid (also known as a uterine leiomyoma, fibromyoma, or fibroid) is basically a smooth muscle tumor originating from the musculature of the uterus (womb).
In the vast majority of circumstances—over 99.7%—it is not cancer. People often tend to associate the word "tumour" with cancer, but in this case, that fear is largely unfounded.
The unique aspect of a fibroid is its variability. They can grow to various sizes—from tiny seedlings to large masses—and can be single or multiple.
This is one of the most common diagnoses on a pelvic ultrasound for women in India, especially during routine check-ups. Often, these fibroids are innocent bystanders; they exist without causing any symptoms.
Their growth is largely driven by the hormonal milieu of your body, specifically estrogen and progesterone. This is why they typically appear during the reproductive years (ages 20-45).
This is one of the main reasons why fibroids are often associated with endometriosis and other disorders that are hormonally dependent.
Are Fibroids a Disease or a Growth?
Fibroids are benign (non-cancerous) growths that develop within the uterus or on its outer surface. They are not a disease or cancer.
In some women, fibroids may cause symptoms such as heavy periods, pain, or a feeling of pressure, depending on their size, number, and location.
While fibroids are rarely life-threatening, they can sometimes affect a woman’s comfort and quality of life, which is why medical guidance is important.
Expert Tip: If you’ve been diagnosed with fibroids, remember that many do not require immediate treatment. As Dr. Jay Mehta, a fibroid specialist in Mumbai, India, often advises, staying informed and scheduling regular follow-ups helps ensure you receive the right care at the right time.
What are uterine fibroids made of?
As described earlier, a fibroid is a growth that arises from the muscle layer of the uterus. It is essentially an abnormal overgrowth of uterine smooth muscle. These muscle fibres grow in a characteristic whorled pattern, forming a compact mass of smooth muscle cells.
This structure allows the fibroid to grow in a circumferential manner and also enables it to receive a blood supply through its surrounding, or peripheral, vascularity.
In very rare situations, the growth of a fibroid may be associated with abnormally high mitotic activity, meaning the cells divide very rapidly. These fibroids tend to behave more aggressively and, in such cases, can develop into a cancerous condition known as a uterine sarcoma.
Are Fibroids Common?
Yes, definitely, fibroids are common.
If you are a healthcare practitioner or even a patient, you’ve likely heard the term "fibroid" often. This is because fibroids are among the most frequently detected findings on routine ultrasound scans.
This disease predominantly occurs in the reproductive age group. That means usually between the age group of approximately 20 to 45 years.
With more people undergoing regular health check-ups today, fibroids are being identified more often than before.
At What Age Do Fibroids Typically Occur?
Fibroids can develop at any age, but they are most commonly seen during a woman’s reproductive years, usually between 18 and 45 years of age. In our clinical practice at Shree IVF Clinic, we often start seeing fibroids more frequently after the age of 27 to 28.
Women in this age group who undergo routine ultrasounds should be aware that finding a small fibroid—sometimes referred to as a “seedling fibroid”—during a regular health check-up is very common.
In fact, this is one of the most frequent incidental findings we see in India, and in most cases, it does not cause any problems.
If you are in your late twenties or older, these seedlings are asymptomatic and do not cause any issues with periods or future pregnancy.
The Growth Phase: 30s to Mid-40s
As women enter their 30s, especially those who have delayed childbearing, the risk of these "seedlings" growing into larger masses (like FIGO 6 or intramural fibroids) increases.
At Shree IVF and Endometriosis Hospital, we find that the demand for surgical intervention peaks in the age bracket of 32 to 42
| Age Group | Common Fibroid Status | Typical Action Required |
|---|---|---|
| 18–25 | Rarely seen | Observation only |
| 26–30 | Seedlings (1–2cm) | Baseline Ultrasound & Monitoring |
| 31–45 | Symptomatic growth | Medical management or Myomectomy |
| Post-Menopause | Shrinkage | Usually no treatment needed |
Not sure if your fibroid needs treatment or just monitoring? Consult with Dr. Jay Mehta for an expert opinion.
Why Do Fibroids Grow During My Reproductive Years?
Fibroids are hormone-dependent, just like conditions such as adenomyosis and endometriosis.
During your reproductive years—roughly between ages 20 and 45—your estrogen and progesterone levels are at their natural peak. Because fibroids thrive on these hormones, this is the time when they are most likely to grow.
This is also why most women in India are diagnosed with fibroids during this stage of life.
However, it’s important to remember that every diagnosis is unique. Many fibroids are small and asymptomatic and may not require surgery or active treatment.
Monitoring hormone-related growth requires a nuanced approach. In many cases, “watchful waiting” is a perfectly valid strategy.
A tailored evaluation helps determine whether your fibroids need active management or simply careful monitoring. If you’re unsure about the next step, you can plan a consultation with Dr. Jay Mehta for a clear, evidence-based assessment of your fibroid growth and overall hormonal health.
Why Are Fibroids Found So Often?
If you’ve been diagnosed with fibroids, try not to panic. Not all fibroids require immediate treatment, and many can be safely managed with regular follow-ups. In many cases, careful monitoring is all that’s needed.
As Dr. Jay Mehta, a fibroid specialist, often explains, understanding the type, size, and location of your fibroids is key to deciding whether simple observation is enough or if treatment may be needed.
The next step is to schedule a follow-up consultation to review your condition in detail, discuss your options, and ensure there is no urgent need for intervention. With the right guidance, you can make informed decisions and choose the approach that best supports your long-term health.
Are fibroids related to hormones?
Yes. Fibroids are hormone-dependent, especially on estrogen.
Estrogen is a normal female hormone produced by the ovaries. In some women, certain uterine muscle cells respond abnormally strongly to estrogen. Instead of behaving normally, one cell starts multiplying and forming a fibroid.
This is why:
- Fibroids usually grow during the reproductive years
- They often shrink after menopause, when estrogen levels fall
Importantly, fibroids are not caused by something you did or didn’t do. They are not due to food habits, stress, exercise, or lifestyle choices.
Patient Tips: Since fibroids are hormone-dependent, our treatment strategies often involve 'tricking' the body into a low-estrogen state.
Whether we use medical suppression to shrink a fibroid before surgery or a hormonal IUD to control bleeding, we are essentially cutting off the fuel supply to the fibroid.
Why does estrogen trigger fibroid growth?
This is something many patients ask me, and it’s an important question.
We know for certain that estrogen plays a key role in fibroid growth. What we are still studying is why some uterine muscle cells react differently to estrogen than others.
In some women, a few muscle cells in the uterus seem to be extra-sensitive to estrogen. Instead of responding in a normal, balanced way, these cells start multiplying more than they should. Over time, this abnormal response leads to the formation of a fibroid.
Even today, medical research has not found one single cause or switch that explains this behavior.
Specialists around the world—including my own work in fibroid care—continue to study how hormones interact with uterine tissue so we can offer even better, more targeted treatments in the future.
If you’ve been diagnosed with fibroids, it doesn’t mean your estrogen levels are “too high.”
More often, it means your uterus is responding differently to normal hormone levels.
That’s why treatment decisions are never one-size-fits-all. The right approach depends on:
- Your symptoms
- The fibroid’s size and location
- Your age and future pregnancy plans
Expert Tip: If you’re worried about fibroid growth or symptoms, an early, focused evaluation makes all the difference.
Understanding how hormones are affecting your body helps us choose the safest and most effective management plan—whether that’s observation, medication, or surgery.
You don’t have to navigate this alone. A clear explanation and the right guidance can take away much of the fear and uncertainty around fibroids.
How do hormones affect fibroid growth?
Fibroids are very sensitive to the hormones estrogen and progesterone, both produced by the ovaries. This is why fibroids tend to grow during a woman’s reproductive years, when these hormone levels are at their peak.
Because of this hormonal link, treatments that temporarily lower estrogen and progesterone can help shrink fibroids and relieve symptoms. Some commonly used medications include:
- Mifepristone
- GnRH Agonists
- GnRH Antagonists
Each of these medications works a little differently, but the goal is the same: to reduce the hormone levels that drive fibroid growth.
It’s important to remember, though, that these treatments don’t make fibroids disappear completely.
They can provide relief from symptoms and reduce the size of fibroids temporarily, but they are not a permanent cure.
For women who are still trying to conceive, hormonal medications are usually prescribed short-term only, because long-term use can affect fertility. After menopause, when hormone levels naturally decline, fibroids often stop growing or even shrink—but they usually do not vanish entirely.
Expert Tip: If you're considering hormonal treatment for fibroids, it's essential to discuss the potential effects on your fertility goals.
Dr. Jay Mehta, an expert in reproductive medicine, can help you navigate these options and create a treatment plan that aligns with your long-term health and family planning objectives.
Can lowering estrogen shrink fibroids?
Lowering estrogen levels can temporarily reduce fibroid size. Certain medications work by suppressing estrogen, and we sometimes use them to:
- Control symptoms
- Improve anemia before surgery
- Buy time in selected situations
However, it’s important to understand that this effect is usually temporary. Once hormone levels return to normal, fibroids often grow back to their original size.
That’s why hormone therapy is not a permanent cure but a short-term management option in carefully chosen cases.
If you’ve been diagnosed with fibroids:
- Don’t panic—they are treatable
- Don’t rely on myths or unverified “hormone-balancing” cures
- Focus on proper evaluation, especially of size and location
In my practice, I often ask patients to notice how their symptoms change with their menstrual cycle. This gives me useful insight into how hormones are influencing the fibroid and helps tailor the right treatment plan.
Take the next step: Understanding why fibroids grow helps you make calmer, more confident decisions.
If you’re experiencing heavy bleeding, pain, bloating, or fertility concerns, an early evaluation makes a real difference.
Final Tip: If you suspect fibroids or are experiencing symptoms like heavy bleeding or pelvic pain, it’s important to seek medical advice early. Book a consultation with Dr. Jay Mehta, who combines expertise in gynecology with a patient-first approach to provide compassionate care.
Book Your Consultation Today With Dr. Jay Mehta, the best doctor for Fibroids in Mumbai, India
Are Uterine Fibroids Genetic? Understanding Your Risk Factors
Many patients ask me if fibroids are inherited, and the answer is not straightforward.
While research shows that some women are more likely to develop fibroids—particularly women of Indian or African descent—there isn’t a single gene that guarantees fibroid development.
Fibroids can behave very differently from one person to another. Some women may develop tiny, asymptomatic fibroids that never cause issues, while others may experience larger, rapidly growing fibroids.
Because of this variability, it’s difficult to establish a clear genetic pattern, and currently, no genetic test can predict with certainty who will develop fibroids.
Expert Tip: If you have a family history of fibroids or belong to a higher-risk group, early screening is important.
I recommend regular ultrasounds to monitor any changes. Detecting fibroids early allows us to manage them proactively, preventing small growths from becoming larger complications.
If you’re concerned about your risk factors, I can provide a personalized assessment and preventive care plan tailored to your health and fertility goals. Book a consultation with Dr. Jay Mehta to understand your fibroid risk and options for early monitoring.
Stress and Fibroids: Is There a Connection?
This is one of the most common questions I hear from young women: “Can stress cause fibroids?”
At present, there is no scientific evidence proving that stress directly causes fibroids.
Many theories circulate on social media and in support groups, but medical research has not established stress as a direct cause of fibroid development.
That said, stress does affect your body in many indirect ways. Chronic stress can influence hormonal balance, immune function, sleep, and pain perception—which may worsen symptoms in women who already have fibroids, even if it doesn’t cause them.
Expert Advice: Taking care of your mental and emotional well-being is an important part of overall gynecological health. Stress-management techniques such as regular exercise, mindfulness, adequate sleep, and emotional support can significantly improve your quality of life.
If you’re experiencing symptoms like heavy bleeding, pelvic pain, or cycle changes, it’s important to focus on medical evaluation rather than self-blame. A proper assessment helps us understand what’s truly happening and plan the right next steps.
Obesity and Fibroid Risk: Is There a Connection?
Many women ask whether being overweight or obese can increase the risk of developing fibroids. This is a thoughtful and valid question.
In women with obesity, there is a tendency for peripheral conversion of hormones—meaning that fat tissue can convert certain hormones into active forms of estrogen.
This additional estrogen circulating in the body may stimulate fibroid cells in some women and contribute to their growth.
However, it’s important to be very clear and reassuring here:
There is no strict or definitive scientific proof that obesity alone causes fibroids.
Fibroids are extremely common, and many women with a healthy body weight develop them, while many women with obesity never do.
What this means for you: Obesity may act as a contributing factor in some cases, but it is not a direct cause. Fibroid development is complex and influenced by multiple factors—especially hormones, genetics, and individual tissue response.
This is why we always look at the entire clinical picture, not just weight, before drawing conclusions or recommending treatment.
Can Small Lifestyle Changes Help Manage Fibroids?
In today’s environment, especially in large Indian cities, many women are exposed to air pollution, environmental toxins, and hormonal disruptors. Naturally, this raises concerns about how lifestyle and surroundings may affect reproductive health.
At present, medical science does not fully understand the exact impact of environmental pollutants on fibroid formation, fertility, or pelvic health.
However, we do know that long-term exposure to poor air quality and certain pollutants can interfere with normal hormonal regulation in the body.
Some researchers believe that these environmental factors may influence how hormones behave, potentially disturbing the normal balance within the pelvis. This disturbance could, in susceptible women, increase the risk of hormone-dependent conditions such as fibroids and endometriosis.
That said, this area is still under active research. There is no conclusive evidence that pollution directly causes fibroids—but it is reasonable to acknowledge it as a possible contributing influence rather than a proven cause.
Fibroids do not develop because of one single reason. Most often, they arise from a combination of hormonal sensitivity, individual biology, and environmental influences.
My approach is always practical and balanced:
- Focus on what is proven (hormones, symptoms, size, location)
- Avoid unnecessary fear or blame
- Create a plan that fits your health goals and fertility plans
Many women live full, healthy lives with fibroids—often without needing any treatment at all.
If you’re concerned about your personal risk factors or lifestyle influences, a focused evaluation can help clarify whether observation alone is sufficient or if active management is needed.
What symptoms do fibroids cause, and how are they treated?
The symptoms of fibroids are primarily determined by their location and size. This distinction is critical and often misunderstood.
At a basic level, a fibroid starts from a single muscle cell in the uterus. That one cell begins to grow differently from the others and slowly forms a non-cancerous lump, which we call a fibroid.
Even today, medical science does not have one single clear answer for why fibroids develop in some women and not others, or why one woman may have one fibroid while another has many. What we do know clearly is that hormones play the biggest role.
For example, a very small fibroid inside the uterine cavity (submucous fibroid) can cause severe menstrual bleeding and intense pain.
On the other hand, a large fibroid growing on the outer surface of the uterus (subserous fibroid) may cause no pain at all and sometimes no symptoms whatsoever.
This is why fibroids should never be judged by size alone.
Common Symptoms of Fibroids
-
Heavy Menstrual Bleeding (Menorrhagia)
This is the most common complaint. It usually occurs when fibroids distort or enter the uterine cavity, especially submucosal fibroids or large intramural fibroids. If untreated, this can lead to severe anaemia, fatigue, and breathlessness.
-
Painful Periods (Dysmenorrhea)
Large fibroids or fibroids undergoing degeneration can cause severe cramping and pelvic pain as the uterus attempts to contract around the mass.
Pressure Symptoms
When fibroids grow large, they can press on nearby organs:
- Pressure on the bladder causes frequent urination
- Pressure on the bowel causes constipation or difficulty passing stools
-
Abdominal Swelling
Very large fibroids can cause visible abdominal distension, often mistaken for weight gain or bloating.
-
Infertility
Fibroids that distort the uterine cavity can interfere with implantation, increase miscarriage risk, or block the fallopian tubes.
-
Back Pain
Fibroids on the back wall of the uterus can press on pelvic or spinal nerves, causing persistent lower back pain.
Patient Tip: If you are soaking more than 3–4 pads a day or feeling constantly tired due to low haemoglobin, please do not ignore it. Treating the fibroid can dramatically improve your energy levels and overall quality of life.
If you notice any of these symptoms, it’s best to consult a gynecologist or a fibroid specialist. Dr. Jay Mehta has extensive experience in evaluating fibroids and offers personalised treatment plans based on each woman’s symptoms and needs.
Why Location Matters More Than Symptoms of a Fibroid?
When I assess fibroids, I don’t just look at whether you have pain or heavy bleeding. I look very carefully at where the fibroid is located and whether it could cause problems in the future.
Understanding Different Types of Asymptomatic Fibroids:
- Subserous Fibroids: These grow on the outer wall of the uterus. Generally, these don't require intervention unless they exceed 5 cm. If they grow larger, they may begin to press against adjacent organs like the bladder or bowel, even if they aren't causing pain or bleeding.
- Intramural Fibroids: Located within the muscular wall of the uterus, these are typically left alone if they are smaller than 3 cm. However, if they begin to distort the endometrial cavity (the inner lining), they can significantly impact your ability to conceive.
💡 Health Tip: If you are diagnosed with an asymptomatic fibroid, start a "symptom diary." Track your cycle length and any new feelings of pelvic pressure. This data is invaluable for your specialist during follow-up scans.
Can I have fibroids without experiencing any symptoms?
Yes—absolutely. It is very common to have uterine fibroids without experiencing any symptoms.
In fact, most women who are diagnosed with fibroids do not have any symptoms at all.
Many of my patients are surprised when an ultrasound shows fibroids, especially when they feel completely normal. This happens because today’s ultrasound machines are very advanced.
They can detect even very tiny fibroids that would never have been noticed earlier.
Having no symptoms does not automatically mean you need treatment—but it also doesn’t mean the fibroid should be ignored.
Why do fibroids cause heavy menstrual bleeding?
This is one of the most common questions I hear in my clinic—and the answer is actually quite simple.
Fibroids usually cause heavy periods for two main reasons, depending on where they are located.
The first reason involves fibroids located right in the center of the endometrial cavity, the inner lining of the uterus, where bleeding occurs. These are called submucous fibroids.
Because of their location, they increase the surface area of the uterine lining. As a result, patients experience heavy menstrual bleeding, even if the fibroid itself is very small.
The second situation involves an intramural fibroid, which is a fibroid present in the muscle of the uterus. If this fibroid is larger than 5 to 6 cm, it is highly likely to disrupt the uterine lining and cause heavy bleeding.
Why Heavy Bleeding Should Not Be Ignored
Heavy menstrual bleeding isn’t just inconvenient—it can affect your overall health.
Ongoing blood loss can reduce your haemoglobin levels and lead to anaemia, causing fatigue, Weakness, breathlessness, and poor concentration
In fact, more than 90% of women who present with this symptom will ultimately require surgical extraction of the fibroid.
How Is Fibroid-Related Heavy Bleeding Treated?
Treatment depends on the type of fibroid:
- Submucous fibroids are usually removed using hysteroscopic surgery, a minimally invasive procedure done through the vagina without any cuts.
- Large intramural fibroids are treated with robotic or laparoscopic surgery, which allows precise removal while preserving the uterus.
While medications may provide short-term relief, they often do not stop the fibroid from growing, and delaying treatment can sometimes affect future fertility.
It's common for patients, especially young, unmarried women, to delay surgery due to social pressures and instead seek medical management. However, this often allows the fibroid to continue growing, which can severely impact future fertility.
💡 Patient Tip: If you're experiencing heavy or prolonged bleeding because of a fibroid, don't delay seeking specialized care. Medical management is often not enough.
Early guidance from an experienced fibroid specialist like Dr. Jay Mehta can help prevent complications such as severe anemia and protect your future fertility with the right treatment plan.
Take the Next Step Toward Relief
Heavy bleeding is often a sign that the fibroid has become symptomatic—and your body is asking for attention, not postponement. Dr. Jay Mehta focuses on a personalized, evidence-based approach to fibroid care, helping you understand all available options clearly and compassionately.
The right diagnosis is the first step toward real relief—and toward regaining control of your health with confidence.
Can Fibroids Cause Pelvic Pain?
Many women with fibroids don’t experience any symptoms at all, but pelvic pain is a common concern for those who do.
The type and severity of pain usually depend on the size and location of the fibroid.
How Fibroids Can Cause Pain?
- Large Fibroids: When fibroids grow significantly, they can create a dull, heavy ache or a feeling of pressure in the lower abdomen simply due to their size.
- Submucosal Fibroids: Fibroids inside the uterine cavity can trigger cramp-like pain. This happens because the uterus tries to contract around these fibroids, similar to strong menstrual cramps.
- Internal Bleeding: Rarely, fibroids may bleed inside their capsule, leading to sudden, sharp, or acute pain.
Important Insight: Pain Isn’t Always Just From Fibroids
In my experience, 30–45% of women with fibroids also have endometriosis, a condition that can cause severe, cycle-related pelvic pain. This is why it’s crucial not to assume all pelvic pain comes from fibroids alone.
What We Recommend: Understanding the true source of your pain is the first step toward real relief. With a thorough evaluation, we can distinguish between pain caused by fibroids, endometriosis, or both—and decide on the safest, most effective treatment.
If you are experiencing pelvic pain or symptoms related to uterine fibroids, consult Dr. Jay Mehta for an expert assessment and a personalized care plan.
Patients seeking pelvic pain treatment in Mumbai , India can benefit from his advanced diagnostic approach and fertility-focused treatment options.
Understanding Fibroid Pain During Pregnancy (Red Degeneration)
Pregnancy can sometimes bring unexpected challenges for women with fibroids. One rare but severe situation is called red degeneration.
This occurs when a fibroid outgrows its blood supply, causing part of the fibroid tissue to die. This can lead to sudden, intense abdominal pain.
How We Manage Red Degeneration
Hospitalization for Pain Relief: Most women with red degeneration need hospital care for pain management. This ensures both mother and baby remain safe and stable.
Emergency Surgery (Rare): In very rare cases—Dr. Mehta typically sees fewer than three such cases a year—some situations require urgent surgery (myomectomy) during pregnancy to provide immediate relief when conservative treatments fail.
What You Should Do
If you are pregnant and experience localized, sharp pain from a fibroid, do not wait. Early evaluation and intervention are key to preventing complications for you and your baby.
Managing fibroids during pregnancy requires specialized expertise. We can create a safe, individualized plan to manage your fibroid and protect your pregnancy. Speak with our expert (1800-268-4000) about a safe management plan for your pregnancy.
Can Fibroids Cause Bloating or Abdominal Swelling?
At Shree IVF and Endometriosis Hospital, many patients come to us complaining that their "tummy feels hard" or that they look "a few months pregnant" despite no change in weight.
This isn't just "gas" or digestive bloating; it is a physical displacement of your internal organs caused by the mass of the fibroids.
When Size and Location Matter
The degree of swelling is usually tied to the specific FIGO classification and the overall dimensions of the growth:
-
The 7–8 cm Threshold: Fibroids often lead to noticeable abdominal swelling once they exceed 7–8 cm. At this size, the uterus grows out of the pelvic cavity and into the abdominal cavity. You may even be able to feel a firm lump through your abdominal wall, especially when lying flat.
-
The "Bulky Uterus" Effect: Even if you don't have one large fibroid, having multiple smaller intramural fibroids can cause a bulky uterus. This increases the total volume of the uterus, leading to a constant feeling of "heaviness" or pelvic pressure.
-
Subserosal Fibroids (FIGO 6 & 7): Because these grow on the outside of the uterus, they have more room to expand into the abdomen. These are the most likely types to cause visible swelling and pressure on the stomach and diaphragm.
- Progesterone Surge: Just before your period, rising progesterone levels can cause the fibroid tissue to retain more water and blood flow.
- The "Heavy" Sensation: This cyclical engorgement explains why many women feel significantly "bigger" or heavier in the week leading up to their period, even if the fibroid hasn't permanently grown in size.
-
Laparoscopic Myomectomy: For large fibroids causing swelling, we can remove the mass through tiny keyhole incisions, allowing your abdomen to return to its natural shape.
-
Medical Suppression: In some cases, we use medications to shrink the fibroids and reduce the "heaviness" before deciding on surgery.
Hormonal Effects and Cyclical Bloating
Fibroids are hormone-sensitive, meaning their activity fluctuates with your menstrual cycle.
What We Recommend at Shree IVF Clinic
If you notice persistent swelling or a heavy feeling in your stomach, it’s important to get a precise assessment from a fibroid specialist to rule out other causes like ovarian cysts or adenomyosis.
💡 Expert Tip:
We often ask our patients to track their bloating alongside their menstrual cycle using a diary.
This helps us determine whether the symptom is caused mainly by the fibroid’s physical size (which requires surgical removal) or by hormonal fluctuations (which might be managed with medical therapy).
An accurate diagnosis at our Mumbai clinic involves a specialized pelvic mapping ultrasound. This allows us to see exactly how much space the fibroids are occupying and whether they are pressing on your bladder or bowels.
Is your bloating constant or cyclical? Schedule a pelvic mapping ultrasound with Dr. Jay Mehta to find out why.
Can Fibroids Cause Frequent Urination?
Yes—fibroids can affect your bladder, and they frequently cause increased, urgent, or frequent urination
This usually happens when fibroids are located on the front (anterior) wall of the uterus or near the cervix. Because the bladder sits so close to these areas, even a small fibroid (around 3–4 cm) can press on it and cause frequent urination.
At our Uterine Fibroid Clinic in Mumbai, we often see patients who initially suspect a urinary tract infection (UTI) or "weak bladder," only to discover that a uterine fibroid is the actual culprit.
Why This Matters: Even if the fibroid is not very large, the pressure on the bladder can significantly affect your daily life. In many cases, surgical removal of the fibroid provides relief and restores normal bladder function.
We often see this issue in younger women, who may also have concerns about fertility. The good news is that fertility-sparing surgery is possible. At Shree IVF and Endometriosis Hospital, we specialize in laparoscopic myomectomy.
- We remove the fibroid through tiny keyhole incisions.
- We preserve the entire uterus.
- We ensure that your chances of conceiving in the future remain intact.
Our Advice
If urinary discomfort, urgency, or frequency is affecting your life, it’s important not to ignore it. A simple pelvic mapping ultrasound at our Mumbai clinic can confirm if a fibroid is the cause.
Early evaluation allows us to tailor the treatment to your needs—protecting both your comfort and your reproductive health.
Consult Dr. Jay Mehta, a leading uterine fibroid specialist in Mumbai, India, to regain your comfort with personalized treatment options
Can Fibroids Cause Back Pain?
Why Fibroids Impact the Back
The location of the fibroid is the most important factor. Back pain is typically associated with fibroids located on the back (posterior) wall of the uterus.
-
Nerve Pressure: When a posterior fibroid grows large, it can press directly against the nerves of the lower back and the sacral plexus.
-
Ligament Stretching: These fibroids can stretch the uterosacral ligaments—the "support cables" that connect your uterus to the base of your spine. This constant pulling often manifests as a persistent, dull ache in the lower back or even "sciatica-like" pain shooting down the legs.
-
Pelvic Congestion: Large fibroids increase the blood flow and weight in the pelvis, leading to a "heavy" sensation that puts mechanical strain on the lower spine.
Why a Proper Diagnosis Matters
It is important to remember that not all back pain is the same. Because the pelvis is home to many overlapping structures, the source of pain can be tricky to pinpoint.
-
Endometriosis: This condition can also cause severe back pain, often by creating adhesions (scar tissue) that pull the uterus toward the bowel or nerves.
-
Adenomyosis: As we discussed, a "spongy," bulky uterus from adenomyosis is frequently linked to deep, radiating back pain during menstruation.
💡 Expert Tip:
If you are experiencing persistent back pain along with other fibroid symptoms, a thorough evaluation is key. Understanding whether your pain comes from a fibroid, endometriosis, or another cause helps us create the most effective treatment plan.
Struggling with unexplained back pain? Discuss your symptoms with Dr. Jay Mehta to identify if a bulky uterus is the cause.
Do Fibroids Cause Anemia?
Yes—uterine fibroids are a leading cause of iron deficiency anemia in women, specifically when they result in heavy, prolonged, or frequent menstrual bleeding.
At Shree IVF and Endometriosis Hospital, we find that anemia is a significant health concern for many women in India.
When you combine nutritional deficiencies with the excessive blood loss caused by a bulky uterus, hemoglobin levels can plummet, leading to severe exhaustion and health complications
We often see patients who have been enduring heavy bleeding for months before seeking help. By the time they come to us, their hemoglobin levels may drop significantly, sometimes below 8 gm%.
In such cases, urgent treatment of the fibroid is usually needed, but we always make sure to stabilize hemoglobin first to ensure a safe and smooth recovery.
How We Help Restore Your Health
After fibroid surgery, most patients’ hemoglobin levels recover within 4–8 weeks. During this time, we recommend iron-rich nutrition and prescribed supplements to rebuild your iron stores and strength.
Can Anemia Affect Fertility?
Anemia isn’t just about fatigue—it can also impact your fertility and overall reproductive health.
If a fibroid is identified as the main cause of anemia, surgical removal is often the most effective solution.
Removing the fibroid allows your iron levels to return to normal, improves your energy, and helps restore your quality of life.
For women planning a family, we usually recommend trying to conceive 4–6 months after surgery, once hemoglobin levels have stabilized.
If heavy periods are leaving you exhausted, weak, or worried about fertility, it’s important not to ignore the problem.
Schedule a consultation with Dr. Jay Mehta to discuss how treating fibroids can restore your energy and support your reproductive health.
What Are the Different Types of Fibroids?

Fibroids are non-cancerous growths that develop in or around the uterus. The type of fibroid is usually determined by where it grows, and this affects the symptoms and treatment options. Here’s a simple breakdown using the global FIGO classification
1. Submucous Fibroids (FIGO 0, 1, 2)
These grow just under the uterine lining and push into the uterine cavity—the space where a baby would implant.
- Symptoms: Even very small submucous fibroids can cause heavy, flooding periods, irregular spotting, and significant fertility issues or miscarriages.
- Our Approach: Because these are inside the cavity, we often remove them via hysteroscopic myomectomy—a specialized procedure with no external cuts on the abdomen.
- Tip: If you are having trouble conceiving or have severe anemia, this is often the culprit
2. Intramural Fibroids (FIGO 3, 4)
These are the most common types and develop within the muscular wall of the uterus. When multiple intramural fibroids are present, they create what is known as a "bulky uterus."
- Symptoms: They may cause pelvic pain, a "heavy" feeling, and bloating. While some stay silent, others can distort the shape of the uterus and cause heavy bleeding.
- Our Approach: We monitor these closely. If they exceed 4–5 cm or distort the cavity, Dr. Jay Mehta may recommend a laparoscopic myomectomy to restore the uterine architecture.
- Tip: Regular check-ups help us decide whether "watchful waiting" is safe or if intervention is needed.
3. Subserous Fibroids (FIGO 5, 6, 7)
These grow on the outer surface of the uterus, expanding into the pelvic or abdominal cavity.
- Symptoms: They rarely cause heavy bleeding but are famous for "pressure symptoms." Depending on their size, they can press on the bladder (frequent urination), the bowel (constipation), or even the diaphragm (hiccups).
- Our Approach: Since these are on the outside, they are ideal for minimally invasive laparoscopic surgery. We "shell" them out to relieve pressure while keeping the uterus intact.
- Tip: If you feel a hard lump in your lower abdomen or have persistent pelvic pressure, a specialist evaluation is essential.
Understanding the type of fibroid you have is the first step toward effective management and peace of mind. Schedule a 3D Pelvic Mapping Ultrasound with Dr. Jay Mehta to evaluate your fibroids and explore the right treatment plan for you.
What are Intramural Fibroids?
An intramural fibroid is a non-cancerous growth located within the muscular wall of the uterus.
The word "intra" means inside, and "mural" refers to the muscle wall. This is the most common type of fibroid found during an ultrasound.
It is very common to find a small intramural fibroid—often less than 1 cm—during a routine check-up.
We call these "seedling fibroids." While seedlings often require nothing more than "watchful waiting," intramural fibroids can grow significantly. In our clinical experience at Shree IVF Clinic, the threshold for intervention usually follows these patterns:
-
Small (<3 cm): Usually asymptomatic, but can cause pain if they are numerous.
-
Large (>4 cm): Typically require surgical management as they are more likely to cause heavy menstrual bleeding, persistent abdominal pain, or pressure.
-
Cavity Distortion: If a fibroid is large enough to "dent" or distort the endometrial cavity (the baby's room), it can significantly contribute to infertility and recurrent miscarriages.
When Is Surgery Needed for Intramural Fibroids?
Surgery is often recommended for intramural fibroids, especially when they cause significant symptoms or affect fertility.
The goal of surgery is always to remove the fibroid while protecting the uterus, especially for women planning future pregnancies. This is why many patients choose minimally invasive surgery performed by a fibroid specialist.
In some cases, a woman may have multiple intramural fibroids scattered throughout the uterus. This can severely distort the uterine anatomy, leading to infertility and making surgical correction necessary.
Operating on intramural fibroids requires a high level of surgical precision. Because they are buried in the muscle, we must minimize bleeding and avoid damaging the healthy surrounding tissue.
At Shree IVF Clinic, we use 'cold-searing' and advanced suturing to ensure the uterine wall heals stronger than it was before.
💡 Expert Tip: If you have been told you have 'multiple fibroids' and are worried about fertility, a detailed 3D mapping can help determine if you need treatment now or if we can safely wait.
What Is a Submucosal Fibroid, and How Can It Affect My Health?
A submucosal fibroid is a non-cancerous growth that develops just beneath the inner lining of the uterus, called the endometrium.
Because of its location inside the uterine cavity, even a small submucosal fibroid can cause noticeable symptoms.
Sometimes, part of the fibroid may extend slightly into the uterine muscle, but what defines it as submucosal is its direct involvement with the uterine cavity.
Many women with submucosal fibroids experience symptoms such as
- Heavy or prolonged menstrual bleeding (menorrhagia)
- Spotting or bleeding between periods
- Difficulty conceiving or repeated pregnancy loss
Why this matters: Submucosal fibroids can distort the uterine cavity, making it harder for an embryo to implant and grow. If you’re facing fertility challenges, a detailed fibroid mapping can help identify whether a submucosal fibroid is the underlying cause.
What Is the Most Effective Treatment for Submucosal Fibroids?
The most effective and fertility-preserving treatment for submucosal fibroids is hysteroscopic myomectomy. At Shree IVF Clinic, we specialize in this "no-cut" surgery.
This is a minimally invasive procedure in which a fine camera is gently passed through the vagina and cervix into the uterus. There are no cuts on the abdomen, which means faster recovery and minimal discomfort.
In my practice, I use advanced hysteroscopic techniques to improve safety and outcomes:
- Bipolar resectoscope: This allows the procedure to be performed using normal saline, significantly reducing the risk of fluid or electrolyte imbalance during surgery.
- Single-use hysteroscopic shaver: To further enhance precision, we often use disposable hysteroscopic shavers. This technology enables precise removal of the fibroid while carefully protecting the basal layer of the endometrium—an essential factor for women who wish to conceive in the future.
The goal is not just to remove the fibroid but to preserve the health of the uterine lining.
What Can You Expect After the Procedure?
One of the most reassuring aspects of hysteroscopic fibroid removal is how quickly patients feel the difference. Many women notice lighter periods from the very next menstrual cycle.
Because the surgery is performed through the natural vaginal route:
- Most patients go home within 24 hours
- Normal daily activities can usually be resumed the next day
- Recovery is typically complete within a few days
Take the Next Step
If heavy periods or fertility concerns are affecting your quality of life, it’s time to look deeper. A focused 3D ultrasound or hysteroscopy can clarify if a submucosal fibroid is the hidden cause of your symptoms.
Consult with Dr. Jay Mehta to explore advanced, fertility-preserving solutions for submucosal fibroids today.
What are subserosal fibroids and when should I worry about them?
Subserosal fibroids are non-cancerous growths that develop on the outer surface of the uterus. Because of where they sit, they often grow quietly and can become quite large before causing noticeable symptoms.
In many cases, women don’t feel anything unusual at all. These fibroids are often discovered by chance—during a pregnancy scan, a routine ultrasound, or a fertility evaluation.
The reassuring part is that subserosal fibroids usually do not affect fertility, as they are located far away from the inner lining of the uterus, where implantation occurs.
You may only start noticing symptoms if the fibroid grows large enough to cause pressure, such as
- A feeling of heaviness in the lower abdomen
- Pressure on the bladder or bowel
- Visible abdominal fullness in very large fibroids
When Is Surgery Needed for a Subserosal Fibroid?
Surgery is generally considered when
- The fibroid exceeds 6 to 7 cm in diameter.
- It causes significant discomfort or pressure symptoms.
- It shows a rapid growth pattern during serial ultrasound monitoring.
Because these fibroids are located on the outside of the uterus, removing them is often more straightforward than other fibroid types. Importantly, the risk of affecting the uterine lining is very low, which is reassuring for women concerned about future fertility.
How Is the Surgery Performed?
Whenever possible, we prefer to remove subserosal fibroids using laparoscopic myomectomy (keyhole surgery). This approach involves small incisions, less pain, minimal scarring, and faster recovery.
For larger fibroids, removing them through small keyhole incisions can be technically challenging.
In such cases, we may use a technique called colpotomy, where the fibroid is safely removed through the vaginal route. This allows even large fibroids to be extracted without enlarging abdominal incisions and helps patients recover more quickly.
Expert Tips:
Subserosal fibroids are often the easiest to treat but the most likely to be overtreated. If a subserosal fibroid is 3 cm and you have no symptoms, we usually leave it alone.
We only step in when the 'bulk' starts affecting your quality of life or organ function. At Shree IVF, our priority is safe, effective removal with the fastest possible return to your normal routine.
If you’ve been diagnosed with a subserosal fibroid and are unsure if you need surgery, it is time for precision mapping. Understanding your options—especially minimally invasive ones—can make the journey far less stressful.
Concerned about a subserosal fibroid? Schedule a consultation with Dr. Jay Mehta (1800-268-4000) to discuss your diagnosis and personalized treatment options.
Understanding Pedunculated Fibroids: What You Should Know
A pedunculated fibroid is a type of non-cancerous uterine growth that is attached to the uterus by a narrow stalk, called a pedicle. This stalk contains the blood vessels that supply the fibroid.
Depending on where the fibroid is located, pedunculated fibroids are broadly divided into two types.
Pedunculated Subserosal Fibroids (FIGO Type 7)
These fibroids grow on the outer surface of the uterus and are connected by a thin stalk. Because they are not embedded in the uterine muscle, they tend to be more mobile than other fibroids.
In many women, these fibroids cause little to no symptoms, especially when they are small. However, as they grow:
- They may become calcified
- They can sometimes be felt through the abdomen
- Larger fibroids—usually 6–7 cm or more—carry a risk of torsion, where the stalk twists and cuts off the blood supply
Torsion can cause sudden, severe pain and is considered a surgical emergency. To prevent this, we often recommend removing larger Type 7 fibroids laparoscopically, even if symptoms are currently mild.
Pedunculated Submucosal Fibroids
These fibroids grow inside the uterine cavity and hang into the endometrial space through a stalk. Because of their location, they are much more likely to cause symptoms such as:
- Heavy or prolonged menstrual bleeding
- Severe cramping
- Fertility issues or recurrent pregnancy loss
In most cases, surgical removal is recommended to restore the normal shape and function of the uterine cavity.
Correctly identifying a pedunculated fibroid—and clearly visualizing its stalk—is extremely important. This requires high-quality ultrasound imaging and experienced interpretation.
At Shree IVF Clinic, we emphasize that many standard scans miss the pedicle, often misidentifying these as ovarian masses or simple intramural fibroids. We use high-definition 3D ultrasound and hysterosonography to confirm the diagnosis. If your imaging results feel "vague," a specialized second opinion is essential.
If you’ve been told you have a pedunculated fibroid—or if your scan results are unclear—getting a precise diagnosis is the first step toward the right care.
Book an advanced diagnostic evaluation with Dr. Jay Mehta to gain clarity and a personalized plan for your uterine health.
Can You Have Multiple Fibroids?
Yes, it’s very common to have more than one fibroid.
Many women have multiple fibroids of different sizes, located in different parts of the uterus. Some may be very small—often called “seedling fibroids”—while others may grow larger over time.
Fibroids usually don’t grow overnight. When they increase in size, it’s often because they were left untreated or not monitored closely. That’s why regular follow-ups are important, even if you feel well.
If you’ve been told you have fibroids and are unsure whether they need treatment, getting a second opinion from a fibroid specialist can help you make the right decision with confidence.
Why Timely Treatment Matters
Delaying treatment for fibroids can lead to complications as they grow larger, potentially impacting your quality of life or fertility. Early diagnosis and thoughtful monitoring can often prevent unnecessary complications.
💡 Doctor’s Advice:
Taking action early doesn’t always mean surgery—but it does mean understanding what’s happening inside your body.
As a specialist in fibroid management and minimally invasive treatments, I offer personalized solutions for fibroids of all types and sizes. Let’s work together to help you regain comfort, confidence, and control over your health.
What Are Seedling Fibroids? Should You Be Concerned?
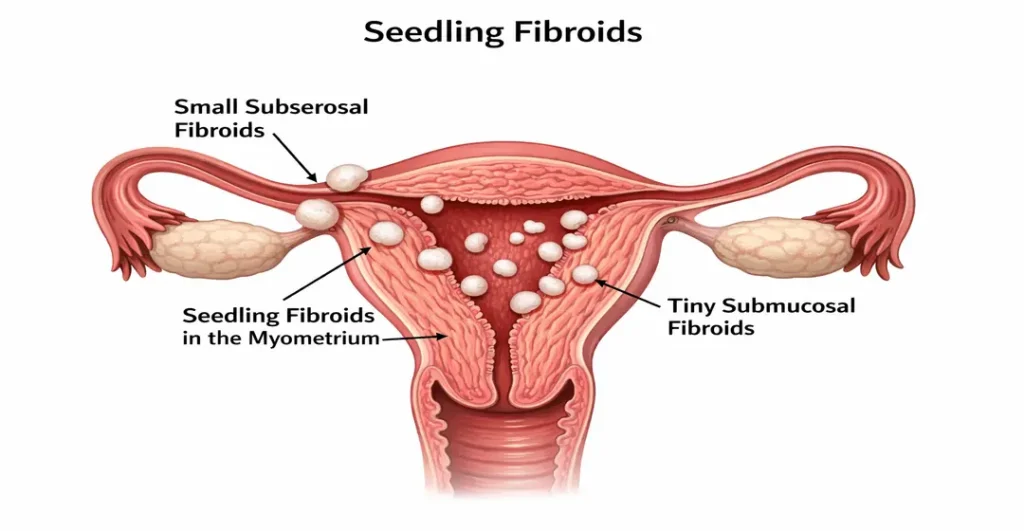
A seedling fibroid is a very small fibroid, usually less than 1 cm in size, often found during routine health checks. Most of these tiny fibroids are harmless and only need an annual follow-up to keep an eye on them.
However, fibroids that are located in the inner lining of the uterus, called submucous fibroids, may have more impact and sometimes need treatment, even if they are small.
If an ultrasound shows a fibroid, it’s always best to consult Dr. Jay Mehta, a trusted gynecologist, to determine whether simple monitoring is enough or if treatment is needed.
Even when fibroids are present, they are usually harmless, especially before menopause. Submucous fibroids after the age of 50 may need closer attention, as most women in this age group are approaching or have reached menopause.
Can Fibroids Cause Infertility?
This is a question I discuss very often with couples who are struggling to conceive, and the answer is yes—but not all fibroids affect fertility.
What truly matters is the size, number, and, most importantly, the location of the fibroid.
Let me explain this.
If a woman has a very small “seedling” fibroid located within the muscle of the uterus (the myometrium), it usually does not interfere with fertility at all. These fibroids are common and, in most cases, harmless when it comes to conception.
However, fibroids that grow inside the uterine cavity, known as submucous fibroids, are a different story. These fibroids directly disturb the lining of the uterus (the endometrium), where implantation occurs.
They are strongly associated with infertility, repeated implantation failure, and heavy menstrual bleeding. For this reason, surgical removal of submucous fibroids is considered the gold standard treatment to improve fertility.
Then we come to intramural fibroids, which sit within the uterine muscle. When these fibroids grow beyond 4–5 cm, they can distort the uterine cavity—even if that distortion is subtle.
Many of these fibroids also have a small submucous component that is not obvious at first glance. In such cases, they can significantly affect fertility and may contribute to recurrent IVF failure or recurrent implantation failure (RIF).
In couples who have experienced multiple failed IVF cycles, it is extremely important to evaluate whether fibroids are contributing to implantation problems.
Addressing these fibroids is often an important step in recurrent implantation failure treatment in Mumbai, India, especially when the fibroid distorts the uterine cavity.
Some fibroids are small in size but poorly placed—for example,
- Fibroids near the cervix
- Fibroids close to the fallopian tube openings
Even though these fibroids may not be large, their location can block sperm movement, egg pickup, or embryo transport, making conception difficult.
That’s why, when fertility is a concern, I place great emphasis on detailed fibroid mapping.
Once we clearly understand the fibroid’s relationship with the uterine cavity and reproductive structures, we can sit down together and discuss the best minimally invasive surgical option if surgery is needed.
In many cases, correcting fibroids that distort the cavity can significantly improve implantation rates and IVF success, which is why fibroid surgery is often considered an important step in the overall management of recurrent implantation failure treatment.
My advice is always individualized. Not every fibroid needs removal, but any fibroid that interferes with fertility should be addressed proactively, and preferably by a specialist who focuses on fertility-preserving, minimally invasive fibroid surgery.
If you have been struggling to conceive and have a diagnosis of a bulky uterus or fibroids, a detailed evaluation is the first step. With the right mapping and fertility-focused surgery, many women conceive successfully even after years of difficulty.
If you are planning a pregnancy or facing recurrent implantation failure after IVF, a detailed fertility evaluation can help identify whether fibroids are affecting implantation.
Book a specialized fertility mapping session with Dr. Jay Mehta to explore advanced options for fertility-preserving fibroid treatment and recurrent implantation failure (RIF) treatment in India.
When Can a Fibroid Affect Fertility?
At Shree IVF and Endometriosis Hospital, we believe that a fibroid diagnosis is never a "stop sign" for motherhood—it is simply a signal that we need a more detailed map of your uterine health.
Even if a fibroid causes no pain or bleeding, it can affect fertility if it changes the shape of the uterine cavity—the space where a pregnancy grows.
When a fibroid pushes into this cavity, it can:
- Make implantation difficult
- Increase the risk of early pregnancy loss
In such situations, we may recommend removing the fibroid surgically to restore the uterus to its natural shape.
Once the cavity is corrected, many women can start trying for pregnancy within 4 to 6 months after surgery.
What We Advise If You’re Planning Pregnancy
If you’ve been told you have “small” fibroids and are planning to conceive, we recommend a detailed evaluation rather than guessing.
💡 Fertility Tip: A 3D ultrasound helps us clearly see whether a fibroid is touching or entering the uterine cavity. This gives us much better information than a routine scan.
A routine ultrasound is often not enough. At our clinic, we use high-definition 3D ultrasound to see exactly whether a fibroid is touching or entering the uterine cavity. This precision mapping tells us if the fibroid is a 'silent bystander' or a 'fertility blocker.'
A fibroid diagnosis does not mean you cannot get pregnant. What matters most is where the fibroid is, not just its size
Key Takeaways for Couples:
-
Location > Size: A 2 cm fibroid in the cavity (submucosal) is often more problematic than an 8 cm fibroid on the outer surface (subserosal).
-
Timing is Everything: Addressing fertility-blocking fibroids before starting IVF or natural conception attempts can save months of emotional and physical stress.
-
Individualized Care: We create the best possible environment for a healthy pregnancy by tailoring the treatment to your specific uterine map
Our goal at Shree IVF and Endometriosis Hospital is 'Uterine Restoration.'
We don't just remove a mass; we rebuild the uterus so it is strong enough to handle the expansion and contractions of a full-term pregnancy.
Seeing our patients hold their healthy babies after a complex myomectomy is the ultimate reward of our specialized approach.
If you’re worried about how a fibroid might affect your fertility, a focused evaluation can bring clarity and peace of mind. Let’s identify whether treatment is truly needed and guide you toward the safest next steps.
Will an asymptomatic fibroid prevent me from getting pregnant?
In many cases, asymptomatic fibroids do not prevent you from getting pregnant.
Most fibroids—even when found on an ultrasound—do not interfere with pregnancy, especially if they are small and located away from the inner cavity of the uterus.
Which Fibroids Affect Pregnancy?
This is an extremely important question, especially for women who are planning a pregnancy or are already pregnant.
At Shree IVF and Endometriosis Hospital, we treat every pregnancy involving fibroids with a strategy tailored to the specific "map" of the uterus.
To be very clear, almost all fibroids can influence pregnancy in some way, but the degree of risk depends largely on their size and location.
The fibroids that worry us the most are
- Large fibroids, and
- Fibroids that distort or occupy the uterine cavity, known as submucous fibroids
These are the fibroids most strongly associated with pregnancy-related complications.
Does pregnancy cure fibroids?
This is a very common myth, and I want to clear it up gently and honestly.
Pregnancy does not cure fibroids.
In fact, the relationship between pregnancy and fibroids is quite predictable and simple. All fibroids grow during pregnancy. In reality, they follow a "Rule of Thirds":
- About one-third (≈33%) shrinks in size
- Another one-third remains the same
- The remaining one-third may increase in size
One well-known pregnancy-related complication is red degeneration of fibroids.
When a fibroid grows too fast, it outgrows its blood supply, causing the tissue to break down internally.
This situation often requires hospital admission and treatment with injectable pain medications. The good news is that, with proper care, most patients settle down without long-term consequences.
It’s also important to understand that large fibroids or multiple fibroids can increase the risk of:
- Recurrent miscarriages
- Preterm delivery
- Bleeding during pregnancy, also known as antepartum hemorrhage
As a rule, we do not advise surgery for fibroids during pregnancy, because the risks usually outweigh the benefits.
However, in rare emergency situations—such as when a fibroid undergoes torsion or severe hemorrhage—surgical intervention may become unavoidable, even during pregnancy.
My advice to women is always this: fibroids should ideally be evaluated and treated before planning a pregnancy, especially if they are large, multiple, or affecting the uterine cavity.
Proper counselling and planning can prevent many avoidable complications and help ensure a safer pregnancy journey.
When fibroids need to be removed, minimally invasive surgery—either laparoscopic or robotic myomectomy—performed by a fibroid specialist offers excellent outcomes.
After such surgery, I usually advise patients to wait about 4 to 6 months before attempting conception, allowing the uterus to heal completely and regain strength.
Many women in India fear that having fibroid surgery will make their uterus "burst" during a future pregnancy. At our fibroid treatment clinic, we want to clear up this misinformation.
In reality, when surgery is performed correctly—using proper surgical planes, meticulous suturing, and complete reconstruction of the uterine wall—the uterus heals beautifully.
Clinical Insight
Uterine rupture is extremely rare if the surgery is done correctly. We use meticulous, multi-layered reconstruction to stitch the uterine muscle back together.
When the surgical planes are respected and the suturing is precise, the uterus heals so strongly that it can safely handle the pressure of a full-term pregnancy.
If you have fibroids and are planning a pregnancy, don't wait for a complication to occur. A proactive evaluation can determine if you are a candidate for a fertility-preserving myomectomy.
Can Fibroids Cause Miscarriage?
Yes, certain types of fibroids can increase the risk of miscarriage, particularly in the early part of pregnancy.
However, once again, the location and size of the fibroid are the most important deciding factors.
The fibroids most clearly linked to miscarriage are submucous fibroids—those that grow inside the uterine cavity.
These fibroids interfere directly with embryo implantation and early placental development, which is why they are one of the most commonly reported causes of early first-trimester miscarriages.
Even relatively small submucous fibroids can have a significant impact because they disturb the uterine lining where the pregnancy is meant to grow.
There are also myometrial (intramural) fibroids, which are located within the muscular wall of the uterus. When these fibroids become large in size, they can contribute to miscarriage as well. This happens because:
- They may distort the uterine cavity indirectly
- Their weight and bulk can compromise the blood supply to the developing pregnancy
- They can alter normal uterine contractions and support
It’s important to understand that not every fibroid causes miscarriage, and many women with fibroids go on to have completely normal pregnancies.
However, if a woman has had recurrent pregnancy loss or unexplained early miscarriages, fibroids—especially cavity-distorting ones—must be carefully evaluated.
In such situations, I strongly recommend detailed fibroid mapping and individualized counselling.
When a fibroid is clearly identified as the cause, surgical removal—performed with a fertility-preserving, minimally invasive approach—can significantly improve pregnancy outcomes.
The key is not panic but precision: knowing which fibroid matters and addressing it correctly.
If you have experienced pregnancy loss and have been told you have a bulky uterus or fibroids, don't wait for it to happen again. A specialized evaluation can provide the answers and the solution you need.
Should Fibroids Be Removed Before Pregnancy?
This is a very common and very valid concern—and the answer depends on which fibroid we are talking about.
If a woman is in her reproductive age group and has:
- A fibroid that distorts the endometrial cavity
- A fibroid located inside the uterine cavity (a submucous fibroid)
- A fibroid that is larger than 5–6 cm in size
Then, in most situations, I strongly recommend removing the fibroid before planning a pregnancy.
Fibroids in these locations or sizes are known to increase the risk of:
- Difficulty in implantation
- Early miscarriages
- Preterm delivery
- Painful pregnancy-related complications
Now, it is also true—and I tell my patients this honestly—that many women do conceive and deliver successfully even without removing fibroids. However, pregnancy in the presence of large fibroids or cavity-distorting fibroids carries avoidable risks.
My role as a doctor is not just to say what is possible but to help you choose what is safest and most predictable.
Fibroids that are small but located at abnormal sites—such as near the cervix or close to the fallopian tubes—also deserve special attention, even if they are not very large. These can interfere with fertility and pregnancy progression in subtle but significant ways.
That is why proper counselling and detailed fibroid mapping are essential before making a decision. When a fibroid is clearly identified as a potential risk, removal before pregnancy is considered the best way to ensure a smoother, safer pregnancy journey.
I always advise women to seek care from the best doctor for fibroid treatment and, whenever surgery is needed, to opt for minimally invasive techniques such as laparoscopic or robotic myomectomy at a centre where these procedures are routinely performed.
A well-planned fibroid surgery, done at the right time and in the right hands, can make a world of difference to pregnancy outcomes—and, most importantly, give you peace of mind as you move forward.
Would you like me to draft a list of specific questions you should ask your doctor during a pre-pregnancy fibroid evaluation? Call 1800-268-4000
Fibroids and IVF Outcomes
This is a very important topic, especially for couples who are planning IUI or IVF and want to maximise their chances of success.
At Shree IVF and Endometriosis Hospital, our goal is to ensure that your IVF journey is successful on the first attempt whenever possible.
One of the most common reasons for unexplained IVF failure is a bulky uterus or a fibroid that was overlooked because it was considered "small."
When are fibroids "safe" for IVF?
As a rule, fibroids do not always need to be removed before IVF. If fibroids are present—even if they are multiple—but do not interfere with or distort the endometrial cavity, we usually do not recommend surgical removal.
However, there are non-negotiable situations.
Irrespective of size, if a fibroid:
- Is located inside the endometrial cavity (submucous fibroid), or
- Distorts the endometrial cavity in any way
Then removal of the fibroid becomes mandatory before proceeding with IVF.
Implantation happens in the endometrium, and a distorted or compromised cavity significantly reduces implantation rates and increases the risk of failure.
Another very important group of patients is women who:
- Have large fibroids, and
- Have had previous fertility failures, whether with IUI or IVF
In such cases, I strongly advise fibroid removal. The logic is simple—before moving on to advanced or experimental fertility treatments, we must first correct the obvious, correctable pelvic cause.
I often see patients being advised immunological therapies after multiple IVF failures. My clear advice is this:
Before considering any form of immunotherapy, the pelvis must be “clean.”
And a clean pelvis means:
- No cavity-distorting fibroids
- No large fibroids affecting uterine anatomy
If a fibroid is present and removal is clearly indicated, surgical correction is essential. Once this is done—preferably through minimally invasive fibroid surgery performed by a specialist—IVF outcomes improve significantly.
In fertility treatment, success comes from precision, sequencing, and doing the right thing at the right time. Addressing fibroids appropriately is often the step that transforms repeated IVF failures into a successful pregnancy.
What is the most effective treatment for fibroids when trying to conceive?
The most effective treatment for fibroids when trying to conceive is surgical myomectomy.
When a fibroid affects fertility, surgical removal is the most effective and reliable treatment.
At present, surgery is the only option that can completely remove the fibroid, restore the normal shape of the uterus, and create the healthiest possible environment for a pregnancy.
I often meet patients who are understandably anxious about surgery and hope to avoid it. Because of this, some choose non-surgical or temporary treatments that aim to shrink the fibroid.
While these options may reduce the fibroid size for a short time, they do not remove the fibroid completely.
Once the treatment is stopped, the fibroid often grows back—sometimes delaying pregnancy further and leading to repeat procedures later.
From a fertility perspective, this delay can be frustrating and emotionally exhausting.
My honest advice as a fibroid specialist: If a fibroid is clearly interfering with implantation, pregnancy, or blood flow to the uterus, removing it surgically offers the best chance of conception.
The goal of surgery is not just removal—it is careful restoration of the uterus so it can safely support a future pregnancy.
In most cases, after proper healing, patients can begin trying to conceive within a few months, with significantly improved confidence and outcomes.
Choosing the right treatment is about protecting both your fertility and your peace of mind. A clear diagnosis and a thoughtful surgical plan can make all the difference.
Why is minimally invasive surgery recommended for fibroids?
When fibroid surgery is needed, minimally invasive techniques are almost always the preferred option. Procedures such as laparoscopic or robotic-assisted myomectomy allow us to remove fibroids with great precision while preserving the uterus.
From a patient’s point of view, the benefits are significant:
- Much smaller incisions
- Less pain after surgery
- Minimal blood loss
- Faster healing and shorter hospital stay
- A quicker return to daily life and fertility planning
Most importantly, minimally invasive surgery allows the uterus to be repaired carefully and securely, which is essential for women who wish to conceive in the future. With expert surgical technique, the uterus heals well and can safely support a pregnancy.
Pro Tip: These procedures require advanced skills and experience. A specialist trained in minimally invasive fibroid surgery can ensure both safety and optimal fertility outcomes.
Next step: If fibroid surgery has been recommended for you, consult an expert who routinely performs minimally invasive procedures. Dr. Jay Mehta can help you understand whether this approach is right for your specific condition.
Fibroids in Young Women
Fibroids are a condition that almost exclusively affects women in the reproductive age group, which is why we commonly see them in young women.
Unfortunately, this diagnosis often brings a great deal of anxiety—not just for the patient, but also for parents and families.
In the Indian social context, I frequently encounter a very specific concern: “Should we avoid surgery until marriage?”
As a specialist, my goal is to replace this fear with scientific clarity. Protecting a young woman's future fertility starts with making medical decisions based on health, not social pressure.
There is a widespread fear that undergoing fibroid surgery before marriage may negatively affect a woman’s future prospects or fertility. I want to address this very clearly and calmly—this fear is largely misplaced.
What truly matters is not when the surgery is done, but how and by whom it is done.
If a fibroid is small and asymptomatic, we often do nothing more than regular follow-up. Surgery is not automatically required just because a fibroid is detected.
However, if a fibroid is large, growing, or causing symptoms, then delaying treatment purely due to social concerns can actually create bigger health and fertility issues later on.
In many young women, a large fibroid will eventually require surgical removal, regardless of marital status. When surgery is clearly indicated, doing it at the right time—before complications arise—is usually the wiser decision.
That is why I strongly encourage young women and their families to consult a fibroid specialist. A specialist can:
- Assess whether surgery is truly needed
- Explain fertility-preserving surgical techniques
- Offer reassurance backed by experience and evidence
When fibroid surgery is performed using modern minimally invasive techniques, with careful reconstruction of the uterus, future fertility and pregnancy outcomes are excellent.
My advice is simple:
I often tell parents that the uterus doesn't know a woman's marital status; it only knows its own health. Delaying necessary surgery can transform a simple procedure into a complicated one.
By choosing a specialist who focuses on fertility preservation, you aren't just treating a 'bulky uterus'—you are protecting her future path to motherhood
If you or your daughter has been diagnosed with fibroids, don't let fear guide your decision. A specialized consultation can provide the reassurance and evidence-based planning you need.
Would you like to schedule a private, sensitive consultation with Dr. Jay Mehta to discuss a personalized health plan?
Fibroids After Menopause
It is not uncommon for a woman who had fibroids during her reproductive years—and did not undergo surgery—to continue having fibroids even after menopause.
In most cases, once menopause sets in and estrogen levels fall, fibroids naturally shrink in size and become inactive. Many women remain completely symptom-free and do not require any treatment at all.
When Should You Be Concerned?
While fibroids after menopause are usually benign (non-cancerous), there are specific "red flags" that require an immediate evaluation by a specialist:
1. Postmenopausal Bleeding
This is the most critical symptom. Bleeding after menopause is never considered normal. Even if you have a known history of submucous fibroids (Type 0, 1, or 2), we must investigate to ensure the bleeding isn't caused by something more serious, such as endometrial hyperplasia or uterine cancer.
2. Growth After Menopause
If a fibroid actually increases in size after your periods have stopped, it is a significant concern. This can sometimes be a sign of a rare condition called leiomyosarcoma (a cancerous growth).
3. Pressure Symptoms
Occasionally, a fibroid may be so large that even after shrinking slightly, it continues to press on the bladder or bowel, causing frequent urination or constipation.
However, there are situations where a postmenopausal woman may come to the hospital with abnormal or postmenopausal bleeding.
The Impact of Submucous Fibroids
There are situations where a postmenopausal woman may experience abnormal bleeding, specifically due to a submucous fibroid (those projecting into the uterine cavity). These can cause:
A submucous fibroid can still cause:
- Postmenopausal spotting or bleeding
- Pelvic discomfort or unusual discharge
- Diagnostic confusion with other uterine conditions
In such cases, surgical removal of the fibroid may be required, even after menopause. This is usually done to:
- Stop bleeding
- Obtain tissue for confirmation
- Rule out any other pathology
The key point to remember is that fibroids after menopause are usually benign, but bleeding after menopause is never considered normal and always warrants proper evaluation.
If you have a history of fibroids and are experiencing postmenopausal spotting or pelvic pressure, it is important to have a specialized ultrasound and evaluation.
Would you like to book a 'Postmenopausal Health Check' with Dr. Jay Mehta to ensure your fibroids remain dormant and healthy? Call 1800-268-4000
What Happens to Fibroids After Menopause?
After menopause, fibroids often shrink and usually become less significant.
However, if a fibroid is large, it may press on nearby organs such as the bladder or rectum. This can cause symptoms like frequent urination or difficulty with bowel movements, in which case surgery may be necessary.
Postmenopausal women should stay alert for any pelvic discomfort or pressure and seek medical advice promptly if symptoms arise.
Can Fibroids Shrink After Menopause?
Yes—fibroids do shrink after menopause in the vast majority of women.
Fibroids are hormonally dependent, especially on estrogen. Once menopause sets in, this hormonal support is withdrawn, and as a result, fibroids usually reduce in size and become inactive.
That is why many women who had fibroids during their reproductive years become completely symptom-free after menopause.
However, there is an important nuance that patients should understand.
After menopause, fibroids often undergo degenerative or calcific changes. This means they can become hard and firm, almost stone-like in consistency.
While they may be smaller, their hardness can sometimes lead to pressure-related symptoms, especially on nearby organs.
In some women, these calcified fibroids may cause:
- Bladder symptoms, such as frequent urination or difficulty emptying the bladder
- Pelvic heaviness or discomfort
- Incidental findings on imaging done for other reasons
So, while fibroids generally shrink after menopause, they don’t always become completely irrelevant. Any new symptoms—particularly urinary issues or postmenopausal bleeding—should always be evaluated properly.
If you have a known history of fibroids and develop new pelvic or bladder symptoms after menopause, don’t ignore them.
A timely evaluation helps us distinguish harmless changes from conditions that may need treatment and ensures continued comfort and safety.
How Are Fibroids Diagnosed?
Fibroids, also called uterine fibroids or leiomyomas, are non-cancerous growths in the uterus.
They can vary a lot—some are tiny and cause no symptoms, while others can grow larger and cause discomfort, heavy periods, or fertility issues.
Accurate diagnosis is the first step toward effective treatment. In my practice, I rely on fibroid mapping, which is a detailed way to examine the uterus and identify each fibroid’s size, location, and relationship to the uterine lining.
This is far more precise than a basic ultrasound and helps me plan the best treatment for you.
Let’s break down the diagnostic process in detail to help you understand how fibroids are detected and what steps you can take.
The Diagnostic Process for Uterine Fibroids
- Medical History and Symptom Discussion
Diagnosis starts with a conversation. We discuss your menstrual patterns and any history of anemia, pelvic pain, or "bulk" symptoms. Understanding your reproductive goals is essential, as a fibroid that is "fine" for someone in menopause may be a "priority" for someone trying to conceive.
- Physical & Pelvic Examination
A gentle pelvic examination can give clues about the presence, size, and position of fibroids.
- High-Definition Fibroid Mapping
This is our specialty. Unlike a routine ultrasound, specialized mapping focuses on the endometrial cavity:
3D/4D Transvaginal Ultrasound: This provides a three-dimensional view of the uterine architecture, showing exactly how much a fibroid is "denting" the cavity.
Saline Infusion Sonography (SIS): Sometimes, we inject a small amount of sterile saline into the uterus during the scan. This expands the cavity, allowing us to see tiny submucosal fibroids that a standard scan might miss.
- MRI (Magnetic Resonance Imaging)
While ultrasound is our primary tool, an MRI is sometimes necessary if:
- You have a very large number of fibroids (adenomyosis vs. fibroids).
- The fibroids are exceptionally large (over 10–15 cm).
- We need to differentiate a benign fibroid from a rare growth (leiomyosarcoma).
If you are struggling with heavy periods, pelvic pressure, or fertility challenges, don't rely on a generic report. A proper "map" is the key to your relief and recovery.
Schedule a high-definition fibroid mapping session with Dr. Jay Mehta to create a personalized plan for your uterine health.
What Tests Are Done for Diagnosing Fibroids?
For diagnosing fibroids, the most important and reliable test is imaging, especially an ultrasound. In some specific situations, an MRI may also be advised if we need more detailed information for planning treatment.
Apart from these imaging tests, there are no specific blood tests required to diagnose fibroids.
Many patients ask me about blood tests—particularly the LDH (lactate dehydrogenase) test—and whether they are necessary.
I want to clearly reassure you that LDH is not a routine test for fibroids. This test is sometimes discussed only when there is a rare concern about a possible cancerous change within a fibroid.
Even in those situations, it’s important to understand that LDH is not a specific or definitive test for diagnosing cancer in fibroids. An elevated LDH level can occur for many reasons and, on its own, does not confirm anything serious.
In my practice as Dr. Jay Mehta, I focus on using the right tests for the right reason. For the vast majority of women with fibroids, imaging alone is more than sufficient, and unnecessary blood tests only add anxiety without improving diagnosis.
A simple takeaway: If you’ve been told you need multiple blood tests to “confirm” fibroids, it’s perfectly reasonable to ask why. In most cases, a well-performed ultrasound gives us all the answers we need.
If you’re feeling unsure or confused about the tests you’ve been advised to take, I’m always happy to help you understand what’s truly necessary—and what isn’t—so you can move forward with confidence.
Is Ultrasound Sufficient for Detecting Fibroids?
Yes, in most cases, an ultrasound is more than enough to detect fibroids.
In my practice, I rely on high-quality ultrasound imaging because it is safe, effective, and gives us a great deal of information—especially when it’s done carefully and interpreted by an experienced specialist.
I use advanced ultrasound software that allows us to perform fibroid mapping. This means I can clearly see where each fibroid is located, how big it is, and how many are present.
This detailed mapping helps me understand your condition better and guide you toward the most appropriate treatment options.
Sometimes, patients have a large number of fibroids—occasionally more than 20.
In these situations, fibroids can grow close together or overlap, which can make counting each one exactly a bit more challenging.
When that happens, we may use AI-assisted tools to help identify and chart each fibroid as accurately as possible. Even in complex cases like these, ultrasound remains a very reliable and informative diagnostic tool.
As Dr. Jay Mehta, I’ve spent many years diagnosing and treating fibroids, and I trust these advanced ultrasound techniques to give my patients clear answers and confidence in their diagnosis.
A quick tip: If you’ve been told you have multiple fibroids, don’t hesitate to ask your doctor about fibroid mapping.
Understanding the size, number, and location of your fibroids can make a big difference in how you feel about your treatment plan.
Can Fibroids Be Missed on Ultrasound?
This is a very common question I hear from patients—and the honest answer is yes, in some situations, fibroids can be missed on ultrasound, especially when they are extremely small.
Very tiny fibroids, sometimes called “seedling fibroids,” may not always be visible on an ultrasound.
Because of their small size (less than 1 centimeter), they can blend in with normal uterine tissue and simply aren’t large enough to be clearly identified on imaging. This is not a limitation of care—it’s a reflection of how early or minimal these fibroids are.
In most cases, these very small fibroids do not cause symptoms and don’t require treatment.
As they grow, they become much easier to detect on ultrasound, and that’s usually when they start to matter clinically.
In my practice, I use high-resolution ultrasound and detailed fibroid mapping techniques to identify fibroids as accurately as possible. However, no imaging test is perfect, and the goal is always to focus on what’s clinically significant—fibroids that are large enough to affect symptoms, fertility, or treatment planning.
As Dr. Jay Mehta, I always reassure my patients that if symptoms persist or change over time, repeat imaging or follow-up evaluation can help us catch fibroids as they evolve.
A reassuring tip: If your ultrasound is normal but you continue to have symptoms, don’t hesitate to follow up. Listening to your body and staying connected with your doctor is the best way to stay confident about your care.
When Is an MRI Needed to Diagnose Fibroids?
In most routine cases, an MRI is not necessary to diagnose or map fibroids. In my practice, advanced ultrasound techniques usually provide all the information we need to accurately understand the number, size, and location of fibroids.
That said, there are a few specific situations where I may recommend an MRI to get added clarity and ensure the best possible treatment planning.
- Complex Localization: An MRI is considered if there is significant ambiguity regarding the exact location of a fibroid, particularly its proximity or relationship to the endometrium (the uterine lining). Precise mapping is vital for planning surgical interventions like myomectomy.
- Transvaginal Ultrasound Limitations: For young or unmarried patients where a transvaginal ultrasound is not clinically appropriate or possible, an MRI provides a non-invasive, high-definition alternative to evaluate large fibroids thoroughly.
- Clarifying Pathology: It is important to note that an MRI does not offer additional diagnostic value over a specialized ultrasound when assessing if a fibroid is cancerous. Standard fibroid pathology rarely requires an MRI for characterization.
As Dr. Jay Mehta, I use MRI selectively and thoughtfully—only when it truly adds value and helps tailor a more precise, personalized treatment plan for my patients.
A helpful tip: If your ultrasound report doesn’t clearly explain where your fibroids are located, it’s perfectly reasonable to ask your doctor whether a pelvic MRI could offer additional clarity for surgical or treatment planning.
Can Fibroids Be Seen on a CT Scan?
Fibroids can sometimes show up on a CT scan, but I generally do not recommend CT scans for diagnosing or evaluating fibroids.
A CT scan uses X-rays to create images of the body. While this can be helpful for many medical conditions, it doesn’t provide the level of soft-tissue detail we need to clearly see fibroids.
As a result, fibroids can blend in with the normal uterine muscle or nearby pelvic structures, making the findings incomplete or unclear.
Because of this limitation, CT scans often don’t give accurate information about the exact size, number, or location of fibroids.
For proper fibroid evaluation and planning treatment, I strongly prefer more specialized and reliable tools like ultrasound or, in select cases, MRI. These options also avoid unnecessary radiation exposure.
As Dr. Jay Mehta, I always emphasize starting with the right imaging test from the beginning. This helps ensure an accurate diagnosis and prevents confusion or delays in care.
An important tip: Sometimes a CT scan is done for another reason—such as abdominal pain—and fibroids are mentioned as an “incidental finding.”
If this happens, don’t rely on that CT scan alone for decisions about treatment. I usually recommend a dedicated pelvic ultrasound to get precise measurements and a clearer understanding of your condition.
Choosing the correct imaging is the first step toward effective treatment. If you’ve had a CT scan that left you with questions or unclear results, I’m happy to review it with you and guide you toward the most appropriate next step for accurate fibroid assessment.
What Is Fibroid Mapping and How Does It Work?
One of the most advanced ways to diagnose fibroids today is through a procedure known as fibroid mapping.
At the fibroid clinic, we don’t just look for fibroids; we "map" them. Fibroid mapping is a specialized diagnostic process that goes beyond simply confirming a growth exists. It creates a detailed 3D blueprint of your uterus, identifying the exact coordinates of every fibroid.
Think of a standard ultrasound as a "photo" and fibroid mapping as a "GPS navigation system" for your surgeon
How Fibroid Mapping Works
This process uses imaging techniques such as ultrasounds or pelvic MRIs, performed by specialists trained in identifying fibroids with precision.
- Ultrasound: A pelvic ultrasound, often the first diagnostic tool used, can identify fibroids by their typical appearance—a well-defined lesion with peripheral vascularity.
Specialists like Dr. Jay Mehta emphasize the importance of an experienced eye to ensure no fibroid is missed, as their appearance is very characteristic on an ultrasound.
- Pelvic MRI: For more complex cases or when additional detail is required, a pelvic MRI can provide a clearer picture. This imaging technique allows for accurate mapping of the fibroid's location, size, and impact on surrounding structures.
Why Is Patient History So Important?
Apart from imaging, understanding your medical history and symptoms is essential in diagnosing fibroids.
Many women with fibroids are asymptomatic, meaning they may not experience any noticeable issues. However, others may report:
- Heavy or prolonged menstrual bleeding.
- Pelvic heaviness or bloating, particularly if the fibroid is large.
- Pain during menstruation.
We advise all patients to share any changes in their menstrual cycle, pelvic discomfort, or other concerns with their healthcare provider.
Even if you are symptom-free, fibroids can sometimes be detected during routine health checkups. Early evaluation helps in timely management and preserves your reproductive health.
If you notice any unusual changes, schedule a consultation with me, Dr. Jay Mehta, for a personalized assessment.
How Do Specialists Identify Fibroids on Imaging?
When I look at imaging studies, fibroids usually stand out clearly. On an ultrasound, they appear as well-defined, round, or oval lesions, often with blood vessels surrounding them.
This pattern is very characteristic, but it does take experience to interpret correctly. That’s why having a specialist review your scans is so important.
For more detailed cases, we sometimes use an MRI. It gives me a precise view of the fibroid’s size, location, and its relationship with the surrounding structures in your uterus. This helps me plan the most effective treatment—whether that’s monitoring, medication, or surgery.
In my practice, I always combine what I see on imaging with a detailed discussion of your symptoms and medical history. It’s this combination of technology and clinical expertise that allows me to make an accurate diagnosis and recommend the right approach for you.
Expert Tip: Always choose a specialist experienced in fibroid diagnosis. Expertise makes a real difference in ensuring your diagnosis is accurate and your treatment plan is safe and effective.
When Should You Get Checked for Fibroids?
In most cases, fibroids are discovered during routine health checkups or because of symptoms like abnormal bleeding or pelvic pressure.
Many women remain unaware of their fibroids until they undergo imaging for unrelated reasons. However, if you experience any of the following, it’s time to consult a gynecologist:
- Persistent heavy menstrual bleeding.
- Noticeable pelvic heaviness or bloating.
- Unexplained fatigue due to blood loss from heavy periods.
Expert Tip: Don’t wait for symptoms to worsen. Schedule a consultation to discuss your symptoms and explore the right diagnostic options. Early evaluation gives you clarity and peace of mind.
Fibroids are a very common condition, and with the right diagnostic tools, we can usually identify and manage them effectively.
Even if you don’t have symptoms, seeing a specialist like me, Dr. Jay Mehta, can help you understand what’s happening and guide you on the best plan for your health.
Staying proactive about your reproductive health makes a real difference. Early diagnosis and the right guidance can help you avoid complications and maintain a healthy, balanced lifestyle.
Do Fibroids Require a Biopsy?
The answer to this question is very, very straightforward.
Fibroids rarely require a biopsy.
In routine cases, we do not recommend any type of biopsy to diagnose a fibroid.
Fibroids are benign growths, and imaging—especially a well-performed ultrasound—is usually more than sufficient to make the diagnosis confidently.
In very rare situations, if a fibroid shows unusual features or has undergone certain degenerative changes, we may need additional confirmation.
Even then, a biopsy is not done beforehand. Instead, we may recommend an intra-surgical biopsy, also known as a frozen section, during surgery.
A frozen section allows us to quickly confirm whether the tissue is indeed a fibroid and to rule out any rare cancerous change while the surgery is in progress.
This approach helps us make safe, informed decisions without exposing patients to unnecessary procedures.
As Dr. Jay Mehta, I strongly believe in avoiding invasive tests unless they are truly needed. For the vast majority of women with fibroids, no biopsy is required at all, and reassurance is often the most important part of care.
Fibroids vs. Adenomyosis: How to Identify and Treat Them Correctly?
One of the most common areas of confusion we see in gynecology is telling the difference between uterine fibroids and adenomyosis.
Even on ultrasound or MRI, these two conditions can look similar, and their symptoms often overlap.
When they are mistaken for one another, patients may receive the wrong treatment, leading to ongoing pain, heavy bleeding, and unnecessary distress.
That’s why, in our practice, we place great importance on making the right diagnosis from the start. Fibroids and adenomyosis behave very differently, and the treatment approach for each is not the same—especially when fertility is a concern.
Clinical Tip: If you suspect fibroids, adenomyosis, or endometriosis, always consult a specialist rather than a general gynecologist for an accurate diagnosis and tailored treatment.
Why It’s Important to Differentiate Between Fibroids and Adenomyosis
Although both conditions affect the uterus, they are fundamentally different.
Fibroids: What We Explain to Our Patients
- Nature: Fibroids are benign (non-cancerous) tumors that grow in or around the uterus. They are completely encapsulated and can often be surgically removed with a high success rate.
- Treatment: Surgical removal (myomectomy) of fibroids is generally effective in providing complete relief from symptoms.
- Outcome: After surgery, most patients experience complete recovery from issues like pain, heavy bleeding, or other fibroid-related symptoms.
- Fertility: In most cases, we are able to preserve the uterus and protect future fertility.
Adenomyosis: A Different Clinical Challenge
- Nature: Adenomyosis involves endometrial tissue growing into the muscular wall of the uterus. Unlike fibroids, it is diffuse and cannot be entirely removed surgically.
- Treatment Challenges: Complete removal of adenomyosis often requires a hysterectomy (removal of the uterus). However, this is not an ideal solution for women in their reproductive years who wish to preserve fertility.
- Symptom Management: Our focus is on controlling pain and heavy bleeding rather than curing the condition.
- Fertility Consideration: Treatment decisions must be made very carefully in women who still wish to conceive.
Fibroids vs. Adenomyosis at a Glance
| Condition | Complete Removal Possible? | Effect on Fertility | Common Treatment |
|---|---|---|---|
| Fibroids | Yes | Fertility can often be preserved post-surgery | Myomectomy |
| Adenomyosis | No | Can impact fertility; requires careful planning | Symptom management or hysterectomy |
When Should You Ask for Diagnostic Clarity?
If you are experiencing:
- Heavy or prolonged periods
- Severe menstrual cramps
- Chronic pelvic pain
- Pain that doesn’t improve despite treatment
I strongly advise asking your doctor one direct question:
“Is this fibroids or adenomyosis? ”,
Advanced imaging, such as high-resolution ultrasound or MRI, allows me to differentiate the two accurately and plan treatment accordingly.
Why Consult a Specialist for Fibroids or Adenomyosis?
General gynecology is not the same as fibroid or adenomyosis expertise. These conditions require:
- Advanced imaging interpretation
- Surgical judgment
- Fertility-focused decision-making
As someone who works extensively with fibroids, adenomyosis, and fertility-preserving surgery, my goal is not just to treat symptoms but to protect your long-term reproductive and hormonal health.
I’m Dr. Jay Mehta, and in my practice I combine careful diagnosis with thoughtful treatment planning, drawing on experience in both gynecological surgery and fertility care.
This approach allows me to recommend options that are medically sound, proportionate, and aligned with what matters most to you—today and in the years ahead.
If you are dealing with fibroids, adenomyosis, or fertility concerns and feel unsure about the right next step, a focused consultation can help bring clarity.
We can review your reports together, discuss realistic options, and decide on a plan that truly fits your body and your goals.
Treatment Options for Fibroids and Adenomyosis
Fibroid Treatment:
- Surgical Removal (Myomectomy): Fibroids are encapsulated, making complete surgical removal achievable in most cases. The result is often a full recovery from symptoms.
- Fertility Planning: Myomectomy is generally safe for patients looking to conceive in the future, provided it is performed by a skilled specialist.
Adenomyosis Treatment:
- Symptom Management: Medications and hormonal therapies may help manage pain and reduce bleeding.
- Surgical Options: For severe cases, a hysterectomy is the only permanent solution. However, this is typically a last resort for women who no longer wish to retain their fertility.
Tip: Always discuss your fertility goals with your specialist before undergoing any surgery for fibroids or adenomyosis. I recommend exploring minimally invasive surgical options when possible to preserve reproductive health.
The Role of Advanced Diagnostic Tools
In our practice, we believe that accurate diagnosis is the foundation of effective treatment.
That’s why we rely on advanced imaging techniques such as 3D ultrasonography and MRI to clearly differentiate between fibroids and adenomyosis. These tools allow us to see the uterus in much greater detail and plan treatment with precision.
Our advice: If you’ve received unclear or conflicting reports in the past, don’t hesitate to ask for advanced diagnostic imaging.
When we understand your condition accurately, we can tailor the treatment specifically to your symptoms, fertility goals, and long-term well-being.
Frequently Asked Questions About Fibroids and Adenomyosis
- Can adenomyosis and fibroids occur together?
Yes. Many women have both, which is why diagnosis can be challenging, and treatment must be individualized.
- Can adenomyosis be cured without a hysterectomy?
While a hysterectomy is the only permanent solution, symptoms can often be managed with medications or hormonal therapies.
- How does surgery for fibroids differ from adenomyosis?
Fibroids can be completely removed through surgery, while adenomyosis often requires symptom management or a hysterectomy for complete relief.
Fibroids and adenomyosis may sound similar, but treating them the same way is a mistake. A precise diagnosis protects your health, prevents unnecessary surgery, and safeguards fertility wherever possible.
Next step: Book a consultation with me, Dr. Jay Mehta, for a clear diagnosis and a treatment plan tailored to your symptoms, uterus, and future goals.
Fibroids vs. Ovarian Cysts: What’s the Difference?
In our clinical practice, we often see women who have both fibroids and ovarian cysts at the same time, which can understandably create confusion.
While both conditions are common, they originate from very different organs and behave differently.
Fibroids are non-cancerous growths that arise from the muscle of the uterus. Ovarian cysts, on the other hand, are fluid-filled sacs that develop on or within the ovaries.
One important overlap we frequently observe is with endometriotic (chocolate) cysts. Fibroids and endometriosis tend to coexist in nearly all cases, which means symptoms may overlap and require careful evaluation rather than assumption.
Clinical Tip: If you’re experiencing pelvic pain, irregular or heavy periods, bloating, or difficulty conceiving, we strongly recommend a specialist evaluation. In many cases, symptoms may not be due to just one condition—fibroids, ovarian cysts, or a combination of both may be contributing.
Accurate imaging and expert interpretation allow us to identify the true cause and guide you toward the most effective, fertility-safe treatment plan.
What About Simple Ovarian Cysts?
In some women, fibroids may coexist with simple ovarian cysts. These cysts are usually related to hormonal imbalance or cycles where ovulation does not occur. In most cases, they are benign, functional cysts and do not pose a long-term health risk.
When we identify a simple cyst, our first step is to understand why it has formed, how large it is, and whether it is changing over time. Many simple cysts resolve on their own or respond well to medical management, without the need for surgery.
This is why an accurate diagnosis is so important. Not every ovarian cyst needs to be operated upon, and unnecessary surgery can sometimes do more harm than good—especially for women concerned about fertility.
Tip: Consider Non-Invasive Options First
In my practice, we always start with conservative, noninvasive treatment for simple ovarian cysts unless there are clear complications such as persistent pain, rapid growth, or suspicion of a non-benign nature.
I strongly advise discussing your scan findings with a trusted specialist so that treatment is guided by evidence—not urgency—and your long-term ovarian health is protected.
Why Specialized Care is Crucial
In India, financial constraints and reliance on nearby clinics often lead women to seek care from general practitioners instead of specialists.
This can result in suboptimal treatment for fibroids and ovarian cysts, further jeopardizing fertility. Seeking expert advice ensures that treatment decisions are clinically sound and focused on long-term health.
In India, I often see women delay or simplify their care because of financial concerns, insurance packages, or the convenience of a nearby clinic. While this is completely understandable, fibroids and ovarian cysts are not conditions that should be managed with a one-size-fits-all approach.
When treatment is guided by a general protocol rather than specialist insight, there is a real risk of incomplete evaluation or unnecessary surgery—both of which can quietly affect fertility over time.
This is especially important when fibroids and ovarian cysts exist together, as their interaction can influence ovulation, uterine health, and future pregnancy outcomes.
In our practice, we focus on precision diagnosis, fertility-aware planning, and long-term well-being, not just short-term symptom relief. Every treatment decision is made after understanding how it may affect your uterus, ovaries, and reproductive goals.
Expert Care Tip: If you’ve been diagnosed with fibroids, ovarian cysts, or both, I encourage you to seek specialized guidance before deciding on treatment.
With the right expertise, many women can avoid unnecessary procedures and choose options that truly protect their fertility.
By understanding how fibroids and ovarian cysts interact—and why specialist care matters—you are better equipped to make informed, confident decisions about your health.
Whether we manage your condition medically or surgically, our priority is always the same: your long-term reproductive health and quality of life.
Why Do Fibroids and Endometriotic Cysts Often Occur Together?
In my practice, I often see women who have both fibroids and endometriotic ovarian cysts. This is not a coincidence.
Both fibroids and endometriosis are estrogen-dependent conditions. This means they grow and thrive in a pelvic environment where estrogen activity is higher or behaves abnormally.
When the body responds excessively or unusually to estrogen, it can trigger multiple hormone-driven conditions at the same time—such as fibroids in the uterus and endometriotic cysts in the ovaries.
This is why we commonly see fibroids and endometriosis coexisting in nearly 35–40% of patients, especially during the reproductive years.
Fibroids vs. Ovarian (Endometriotic) Cysts:: A Simple Comparison
| Feature | Uterine Fibroids | Ovarian Cysts |
|---|---|---|
| Where they develop | In the muscle of the uterus | On or inside the ovaries |
| Nature of the condition | Solid, non-cancerous muscle growths | Fluid-filled sacs |
| Hormonal dependence | Strongly hormone-dependent (estrogen & progesterone) | Some cysts are hormone-related; others are not |
| Common types | Submucosal, intramural, subserosal, pedunculated | Functional cysts, endometriotic (chocolate) cysts, dermoid cysts |
| Nature of the condition | Solid, non-cancerous muscle growths | Fluid-filled sacs |
| Effect on periods | Heavy, prolonged, or painful periods are common | Periods may be irregular or normal, depending on cyst type |
| Impact on fertility | Can affect implantation or pregnancy if they distort the uterine cavity | May affect ovulation or fertility, especially with endometriosis |
| Pain pattern | Pressure, heaviness, pelvic pain | Sharp pain, dull ache, or sudden pain if cyst ruptures or twists |
| Chance of coexisting conditions | Often coexist with endometriosis (≈35–40%) | Commonly seen with endometriosis |
| Best diagnostic tools | Fibroid mapping ultrasound, 3D ultrasound, MRI | Pelvic ultrasound, Doppler, MRI when needed |
| Definitive treatment | Myomectomy (minimally invasive surgery when needed) | Observation, medication, or surgery depending on type and size |
| Can it disappear on its own? | No | Some functional cysts may resolve spontaneously |
What We Focus on Clinically
We don’t just ask whether fibroids or ovarian cysts are present—we focus on how they are interacting with each other.
A fibroid may alter the uterine cavity, while an endometriotic cyst can affect ovulation or distort pelvic anatomy. When these conditions coexist, they can quietly compound fertility challenges if not evaluated together.
That’s why we rely on advanced imaging, detailed fibroid and ovarian mapping, and hormone-aware clinical planning before recommending any treatment. Our goal is always to understand the complete picture—not just isolated findings.
If you’ve been diagnosed with fibroids, ovarian cysts, or both, it’s important not to view them as separate problems. These conditions often share a common hormonal background, and addressing them together allows us to create a treatment plan that protects both your fertility and long-term pelvic health.
Expert Tips: I always recommend a comprehensive pelvic evaluation, which may include a high-resolution ultrasound or MRI, to clearly identify the presence and impact of both fibroids and ovarian cysts. This approach helps avoid delays, misdiagnosis, and unnecessary treatments.
Can Surgery for fibroids and ovarian cysts impact fertility?
Yes—surgery can impact fertility if it isn’t planned and performed carefully.
At Shree IVF Clinic, we don't just "operate." We plan your surgery with your future family in mind.
When we operate for fibroids or ovarian cysts, our primary responsibility is not just to remove the disease but to protect your reproductive potential.
This becomes even more important when fibroids and endometriotic cysts coexist. An inadequately planned or aggressively performed surgery can unintentionally damage the uterus, ovaries, or surrounding pelvic structures—making conception more difficult later.
I often see women who have undergone surgery at general clinics or under insurance-based packages, where the focus may be on completing the procedure rather than preserving fertility. Unfortunately, once surgical damage occurs, it cannot always be reversed.
We always emphasize that surgeries for fibroids and endometriotic cysts should be performed only by specialists trained in reproductive and fertility-preserving surgery.
The technique, precision, and understanding of pelvic anatomy make all the difference.
Expert Tip: If you’re considering surgery, don’t hesitate to seek a reproductive health expert rather than a general practitioner. The right specialist will tailor the surgery to your condition, your age, and—most importantly—your future fertility goals.
Fibroids and Endometriosis: What’s the Connection?
Many women ask me why fibroids and endometriosis are often mentioned together—and it’s a very valid question.
Fibroids and endometriosis are two of the most common gynecological conditions we see in women of reproductive age. In my clinical practice, I frequently find that both conditions can coexist in the same patient, especially in younger women.
The common link between them is hormones, particularly estrogen. When estrogen acts abnormally within the pelvis, it can stimulate:
- The growth of fibroids in the uterus, and
- The development of endometriosis outside the uterus
This shared hormonal environment can lead to symptoms such as pelvic pain, heavy or irregular periods, bloating, and sometimes difficulty conceiving. Because their symptoms often overlap, one condition can sometimes mask the other unless we look carefully.
A Gentle Reminder from Clinical Practice
If you’re experiencing persistent pelvic pain, painful periods, or unexplained menstrual changes, we shouldn’t assume there is only one cause. A thorough evaluation helps us understand whether fibroids, endometriosis, or both are contributing to your symptoms.
Early and accurate diagnosis allows us to plan treatment that is effective, fertility-aware, and tailored specifically to your body, rather than treating symptoms in isolation.
Why Is Specialized Care Important for Fibroids and Endometriosis?
I often see women who have struggled for years with fibroids or endometriosis, sometimes even after having surgery, yet their symptoms persist.
This situation is usually because these conditions are complex, and not every healthcare provider has the specialized training needed to manage them effectively.
That’s why seeking care from a specialist is so important. As a doctor who focuses on fibroids and endometriosis treatment in India, I ensure that every patient receives a personalized treatment plan that addresses the root cause of their symptoms, not just temporary relief.
Patients looking for an experienced endometriosis doctor in India often come to me after trying different treatments without success.
My goal is to provide comprehensive evaluation and advanced treatment options that improve both symptom relief and reproductive health.
Why You Might Choose My Care for fibroids or endometriosis
Dr. Jay Mehta focuses on treating complex gynecological conditions with precision, personalized care, and fertility preservation.
- Advanced Surgical Expertise
I use advanced minimally invasive surgical techniques designed to remove fibroids and endometriotic lesions with high precision, helping patients recover faster while preserving reproductive health.
Many women seeking endometriosis treatment in India benefit from these modern approaches, which aim to reduce pain, remove the disease effectively, and prevent recurrence.
- Personalized Treatment Plans
Every treatment plan is tailored to you.
- Symptoms and pain severity
- Reproductive goals
- Medical history
- Overall health condition
This personalized approach ensures that women receiving fibroid and endometriosis treatment in India receive care that truly fits their individual needs.
- Expertise in Complex and Recurrent Cases
I have extensive experience managing challenging or recurring cases of fibroids and endometriosis, including patients who have previously undergone surgery but still experience symptoms.
For many patients searching for an endometriosis specialist in India, a thorough reassessment and specialized treatment plan can make a significant difference in symptom control and fertility outcomes.
Expert Tip: If you’ve had surgery before or tried treatments that didn’t fully work, it’s never too late to seek a second opinion from an experienced endometriosis doctor in India.
Together, we can map out the best strategy for long-term symptom relief and improved reproductive health.
Is it Fibroids or Pelvic Inflammatory Disease (PID)? Understanding the Difference
In the Indian healthcare landscape, it is common to see women diagnosed with both uterine fibroids and Pelvic Inflammatory Disease (PID) simultaneously. However, it is vital to understand that these are two distinct conditions with separate origins and different impacts on your health.
How Fibroids and PID Differ
- Uterine Fibroids: These are non-cancerous growths that develop in or on the muscular walls of the uterus. Fibroids are mainly influenced by hormones like estrogen and progesterone, as well as genetic factors.
- Pelvic Inflammatory Disease (PID): This is an infection of the female reproductive organs, often caused by bacteria spreading from the vagina to the uterus, fallopian tubes, or ovaries.
Why This Matters in India
As a renowned expert in reproductive health, Dr. Jay Mehta notes that Pelvic Inflammatory Disease (PID) is particularly prevalent in lower socio-economic regions of India.
This is often linked to limited awareness about proper genital hygiene and restricted access to quality healthcare resources. In contrast, uterine fibroids are a common biological condition that can affect women across all demographics, regardless of socioeconomic status.
| Feature | Uterine Fibroids | Pelvic Inflammatory Disease (PID) |
|---|---|---|
| Nature | Benign (non-cancerous) tumors. | Infection and inflammation |
| Primary Cause | Hormones (Estrogen/Progesterone) | Bacterial infection (often STIs or hygiene-related) |
| Pain Type | Usually heavy pressure or dull ache. | Acute, sharp pelvic pain often with fever |
| Treatment | Hormonal therapy or surgical removal. | Course of antibiotics |
Expert Tip: If you are experiencing persistent pelvic discomfort, it’s crucial not to self-diagnose. PID is an active infection, and delaying treatment can lead to scarring, infertility, or other complications. On the other hand, fibroids are structural growths that require a completely different approach.
Next Steps: The first step toward relief is understanding the cause of your symptoms. If you’re unsure whether it’s fibroids, PID, or both, consult a specialist like me, Dr. Jay Mehta. Together, we can create a clear diagnostic plan and recommend the right treatment for your health and future fertility.
Are Fibroids Cancerous?
The possibility of a fibroid turning into a cancer (called leiomyosarcoma) is extremely rare, usually less than 0.3%.
In my entire career spanning over 13 years, I have operated on very few such cases (about 15 cases) of Leiomyosarcoma (a cancerous fibroid).
While we always stay vigilant for warning signs—like rapid growth or abnormal vascularity seen on Doppler ultrasound—you should not let the fear of cancer dominate your decision-making.
Usually, the growth of the fibroids is abnormally fast when it is about to turn into a malignancy or a cancerous fibroid, like a sarcoma. There are also some other features that we as clinicians notice in ultrasound.
Expert Tip: A fibroid diagnosis does not mean something serious. Most fibroids are completely benign and very manageable. What matters first is knowing what kind of fibroid you have and whether it is affecting you in any way.
If you’re unsure or worried about your diagnosis? Let’s clarify your report and what it means for you. Book a consultation to understand your diagnosis—call 1800-268-4000
Understanding the Difference: Fibroids vs. Leiomyosarcoma
To clarify the key distinctions, here is a simple comparison:
| Feature | Uterine Fibroids (Leiomyomas) | Uterine Cancer (Leiomyosarcoma) |
|---|---|---|
| Nature | Benign (non-cancerous) growths | Malignant (cancerous) tumors |
| Prevalence | Very common | Extremely rare (<0.5% of fibroids) |
| Growth Rate | Usually slow | Often rapid and aggressive |
| Treatment | Varies (monitoring, medication, surgery) | Primarily aggressive surgery; chemo/radiation have limited success |
| Prognosis | Excellent | Challenging due to aggressive nature |
Most fibroids are harmless, and you shouldn’t panic if you’ve been diagnosed. The main differences I look for in my practice are the growth rate and the ultrasound or MRI features.
Rapidly growing fibroids, unusual blood flow patterns, or atypical appearances are the ones that warrant closer evaluation.
Expert Tip: If you notice your fibroids growing quickly or have new symptoms, it’s always worth a detailed review with a specialist. Early assessment helps us distinguish between a typical fibroid and something rare like a leiomyosarcoma, giving you clarity and peace of mind.
What Is STUMP (Smooth Muscle Tumour of Unknown Malignant Potential)?
STUMP is a rare type of uterine smooth muscle tumor that can sometimes develop when someone has abnormal or multiple fibroids. The tricky part about STUMP is that it’s hard to classify as either completely benign (non-cancerous) or malignant (cancerous).
Because of this uncertainty, careful and regular follow-up with your doctor and a pathologist is very important.
If you’ve completed your family and are diagnosed with STUMP, I may recommend a hysterectomy, which usually includes removing the uterus and sometimes the fallopian tubes and ovaries, to reduce the risk of recurrence or any potential spread.
Expert Tip: Being diagnosed with STUMP can feel overwhelming, but seeking a second opinion is often helpful. It allows you to understand your options fully and make decisions with confidence.
If you’ve been diagnosed with multiple fibroids or a STUMP tumor, you can schedule a consultation with Dr. Jay Mehta to review your case and plan the best long-term approach for your health.
How Does a Cancer Suspicion Affect My Surgery?
If there’s ever a suspicion of cancer before or during fibroid surgery, I immediately adjust the surgical plan to ensure your safety.
- Open Surgery (Laparotomy): The procedure is immediately converted from a minimally invasive surgery (laparoscopy) to an open surgery (laparotomy). This allows me to remove the tumor carefully without risking the spread of any potentially cancerous cells.
- Uterine Conservation May Not Be Possible: In these rare cases, preserving the uterus is not the safest option. My priority becomes removing the entire tumor safely to protect your long-term health.
I understand this can feel overwhelming, but please know that these steps are taken strictly as a safety measure. With experience in complex fibroid and uterine surgeries, I make these decisions in the operating room to ensure your best outcome and peace of mind.
How do doctors identify cancerous fibroids?
Doctors use various tools to identify fibroids that may be cancerous, such as ultrasounds or, in some cases, MRI scans. Suspicious signs include:
- Rapid growth of the fibroids.
- Poorly defined capsule around the fibroid.
- An abnormally high blood supply (vascularity) within the fibroid.
While MRI scans and Doppler ultrasounds can provide valuable clues, they are not definitive diagnostic tools.
Expert Tips: Speak with your doctor if you notice rapid changes in fibroid size or experience new symptoms. A tailored diagnostic plan is the best way to address any concerns.
Is Pre-Surgical Testing for Fibroid Cancer Accurate?
Before surgery, certain tests may be advised to assess the risk of a cancerous fibroid. Blood tests such as serum LDH (lactate dehydrogenase) levels are sometimes used, but it’s important to understand that they are not specific or definitive for diagnosing fibroid cancer.
Similarly, Doppler ultrasound scans can help identify unusual blood flow patterns around a fibroid by measuring parameters like peak systolic velocity (PSV). While these findings may raise suspicion, they are supportive tools only and cannot confirm cancer on their own.
Expert Tip: If you have been diagnosed with fibroids, remember that the risk of cancer is extremely low. Most fibroids are benign and can be safely monitored. Regular follow-ups and honest discussions with your doctor play a crucial role in effective management.
In the rare situation where a cancerous fibroid is suspected, detailed counselling and discussion within a tumour board are essential to ensure the safest and most appropriate treatment approach.
Before any surgery, it is always advisable to be evaluated by a multidisciplinary team. Seeking a second opinion can also provide clarity, reassurance, and confidence in your treatment plan.
Are MRI and Blood Tests Reliable for Detecting Cancer in Fibroids?
I often get asked whether tests like MRI scans or blood markers, such as LDH, can tell if a fibroid is cancerous. The truth is, these tools are helpful but not definitive. They can suggest areas of concern, but they don’t always give a clear answer.
The final confirmation usually comes from examining the tissue under a microscope after surgery. That’s why I emphasize a comprehensive evaluation rather than relying on a single test.
Take the Next Step: If you’re worried about your fibroids, it’s important to consult a specialist who can look at your full clinical picture—including imaging, symptoms, and your history—not just individual test results. I can guide you through this process and ensure we take the safest, most informed approach.
What Happens During Surgery for Cancerous Fibroids?
In the rare situation where cancer is suspected during surgery, it may be safer to change from a laparoscopic or minimally invasive procedure to an open surgery through a vertical incision.
This ensures that all recognised cancer surgery protocols are followed, which is essential when treating a cancerous fibroid, called a leiomyosarcoma.
One of the warning signs seen during surgery is an enlarged infundibulopelvic (IP) ligament, which may be due to increased blood supply to the fibroid and can raise suspicion of cancer.
Confirmation is done during surgery using a frozen section biopsy, where a small tissue sample is examined immediately to guide further surgical decisions.
In most cases, if cancer is confirmed, a hysterectomy with bilateral salpingo-oophorectomy is performed. This involves the removal of the uterus, fallopian tubes, and ovaries to ensure complete removal of all cancerous tissue
Expert Tip: If surgery is planned, a pre-surgical consultation is important. It allows you to discuss the procedure, recovery, and outcomes in detail, helping build clarity, confidence, and trust.
How Are Uterine Fibroids Treated?
The majority of fibroids that I see in women—especially in India—are small in size or completely asymptomatic. These fibroids usually do not need any active treatment.
In such cases, the most common and appropriate approach is observation. This simply means a yearly follow-up visit with a fibroid specialist after accurate fibroid mapping has confirmed the size and location of the fibroid.
This “watch and monitor” approach is the most common treatment for fibroids and is perfectly safe when there are no symptoms.
A helpful tip: If you’ve been diagnosed with small, asymptomatic fibroids, regular monitoring is usually all that’s needed. I recommend an annual follow-up with a specialist so we can track any changes over time and keep things under control.
This simple step often provides reassurance and helps ensure long-term peace of mind.
When Should Fibroids Be Treated?
Once fibroids are diagnosed and start causing symptoms, treatment should be considered without unnecessary delay—provided you are medically fit for surgery. Symptoms such as pain, heavy menstrual bleeding, or fertility problems usually indicate that the fibroid is affecting your health and should not be ignored.
When surgery is recommended, it is extremely important that it is performed by a doctor who specialises in fibroid management. The way fibroids are removed plays a major role in protecting the uterus and preserving long-term reproductive potential, especially for women who wish to conceive in the future.
As Dr. Jay Mehta, I place great emphasis on precision, uterine preservation, and minimally invasive techniques whenever possible. A well-planned and expertly performed surgery not only relieves symptoms but also supports better long-term outcomes.
A key message to remember: the right timing and the right surgeon matter. Careful surgical management can make a meaningful difference to both recovery and future fertility.
If you’ve been told you have symptomatic fibroids and are unsure about the next step, seeking specialist guidance early can help you make a confident and well-informed decision.
Can Fibroids Be Treated Without Surgery?
This is an important question, and I always like to answer it honestly and clearly.
Non-surgical treatments for fibroids do not offer a permanent cure. They usually lead to only a temporary reduction in fibroid size and are best reserved for special situations—mainly when a patient clearly needs surgery but is medically unfit to undergo an operation.
When patients or their families consider non-surgical options, it’s very important that they are thoroughly counselled and understand that these approaches are not definitive treatments. They may help for a short period of time, but the fibroid itself is not permanently removed.
One such option is Uterine Artery Embolisation (UAE), which is performed by an interventional radiologist. While UAE can reduce fibroid size, it comes with its own set of risks and is known to significantly compromise fertility.
Because of this, I generally do not recommend UAE for women in the reproductive age group or those who wish to preserve future fertility.
I also want to address something I see quite often in India. There are many practitioners of alternative or non-medical therapies who claim they can “cure” fibroids without surgery.
I strongly advise patients to exercise caution with such claims. At present, there is no scientifically proven alternative treatment that can permanently eliminate fibroids.
As Dr. Jay Mehta, my priority is always your long-term health and safety. I encourage patients to ask questions, do their own research, and make informed decisions based on evidence—not marketing promises.
Key takeaway: Non-surgical treatments may have a limited, temporary role in select patients, but surgery remains the most reliable and curative option when fibroids need treatment.
If you’re unsure which approach is right for you, a detailed consultation can help you understand your options clearly and confidently.
Which is the best treatment for fibroid surgery?
Surgery (laparoscopic or robotic myomectomy) is usually recommended when fibroids start causing symptoms that affect your health or quality of life.
In my practice, fibroids are considered symptomatic when they lead to problems such as:
- heavy or prolonged menstrual bleeding
- persistent pelvic or abdominal pain
- difficulty conceiving, or recurrent miscarriages
- pressure on nearby organs, such as the bladder or bowel
There are also situations where fibroids are large but not yet causing symptoms. Fibroids that are typically larger than 6–7 cm, even if asymptomatic, often need surgical removal.
Over time, their size can lead to pressure on the bladder—causing frequent urination—or on the bowel—leading to constipation. If left untreated, this pressure can eventually interfere with normal organ function.
As Dr. Jay Mehta, I specialise in minimally invasive surgical techniques for fibroid removal.
These approaches are designed to reduce pain, scarring, and recovery time while still achieving excellent outcomes. The most commonly used options include:
- Laparoscopic Myomectomy – Fibroids are removed through small keyhole incisions in the abdomen.
- Robotic-Assisted Myomectomy—A highly precise technique using robotic assistance for enhanced vision and control, especially helpful in complex cases.
If you are experiencing symptoms or have been told you have large fibroids, discussing your surgical options is an important next step.
Understanding when surgery is needed and which approach is best can make the decision much less overwhelming.
What is a myomectomy?
When a fibroid needs treatment, the surgery we most commonly recommend is called a myomectomy. The word itself is quite simple—"myoma" means "fibroid," and "ectomy" means "surgical removal."
So, a myomectomy is the surgical removal of the fibroid while preserving the uterus.
In this procedure, the fibroid is completely enucleated, meaning it is carefully separated and removed from its fibroid bed without damaging the uterus.
The goal is always to preserve the uterine cavity in its entirety, especially in women who wish to retain fertility or simply want to keep their uterus.
Once the fibroid is removed, the most critical step of the surgery follows. The fibroid bed is sutured very meticulously, layer by layer, so that:
- The cavity is completely closed
- There is no internal blood collection (hematoma)
- The uterus regains its natural strength
This careful reconstruction allows the uterus to heal completely and plays a vital role in ensuring safe future pregnancies.
Myomectomy is considered the treatment of choice whenever a fibroid becomes symptomatic or requires intervention.
It can be performed either as an open surgery or through minimally invasive techniques, such as laparoscopic or robotic surgery.
While the surgical approach may differ, the principles of surgery always remain the same—precise fibroid removal and strong uterine reconstruction.
In cases where the fibroid is located inside the uterine cavity, known as a submucous fibroid, the surgery is usually performed via a hysteroscopic myomectomy.
In this technique, a small camera is introduced through the cervix into the uterus, and the fibroid is removed without any external cuts.
As a fibroid specialist, my focus is not just on removing the fibroid but on doing it correctly and permanently while safeguarding the uterus and the patient’s long-term reproductive health.
Laparoscopic Myomectomy : How It Works
When fibroids are removed using keyhole surgery, the procedure is called a laparoscopic myomectomy.
As a fibroid specialist and part of a unit of excellence for advanced endoscopic surgery in India, this is a surgery that we perform very routinely, and we see patients travel from across the country specifically for this expertise.
In laparoscopic myomectomy, we place a high-definition camera—preferably a 3D camera—inside the abdomen.
Through a few very small ports, the entire surgery is performed using specialised laparoscopic instruments.
Despite being minimally invasive, the principles of surgery remain uncompromised—the fibroid is completely removed, and the uterus is carefully reconstructed.
Once the fibroid is enucleated from its bed, the most important step is suturing the uterus properly. This is not a basic skill—it requires a high level of expertise in laparoscopic suturing.
In our practice, we routinely use barbed sutures, which allow even distribution of tension across the uterine wall and promote excellent healing without the need for multiple knots.
To minimise blood loss during surgery, we prefer a technique where the uterine arteries are temporarily clipped, reducing blood flow only for the duration of the procedure.
Some surgeons use diluted vasopressin injections for the same purpose, but we consciously avoid this because of the potential cardiac side effects, and our anesthesia team prioritises patient safety above all else.
Another important aspect of laparoscopic myomectomy is specimen removal.
We do not prefer power morcellation. Instead, whenever the patient permits, we remove the fibroid through a small vaginal incision, which is cosmetically excellent and avoids unnecessary abdominal extension.
From a surgeon’s perspective, I personally prefer operating through the central (middle) port, as it allows natural shoulder movement and greater precision—something that becomes very important in complex laparoscopic procedures.
Because the incisions are very small, recovery after laparoscopic myomectomy is remarkably fast.
Most of our patients are comfortable, mobile, and ready to go home within 24 hours of surgery.
In experienced hands, laparoscopic myomectomy offers the best balance of complete fibroid removal, uterine preservation, faster recovery, and excellent long-term reproductive outcomes.
Hysteroscopic Removal of Fibroid (Hysteroscopic Myomectomy)
Hysteroscopic fibroid removal is a technique that we typically use for submucous fibroids, especially those that are within the uterine cavity and usually up to about 4 cm in size.
In this procedure, a small camera is gently passed through the vagina and cervix into the uterus, so there are no cuts on the abdomen at all.
Once we visualise the fibroid, we remove it using specialised instruments. These may include a bipolar resectoscope or a hysteroscopic shaver.
In our practice, we use both when indicated, but in the vast majority of cases, we prefer the hysteroscopic shaver.
The reason is simple—it allows the fibroid to be removed quickly, smoothly, and without the use of electrical current, which adds an extra layer of safety.
This also means less thermal damage to the surrounding endometrium, which is especially important for women who are planning future pregnancies.
Recovery after hysteroscopic fibroid removal is extremely fast. Most patients are comfortable and ready to go home within 4 to 6 hours of the procedure.
One of the most critical aspects of good hysteroscopic surgery is patient safety, particularly maintaining careful control over uterine distension.
We deliberately work with minimal distension pressures, which significantly reduces fluid absorption and the risk of water retention–related complications.
When performed by an experienced surgeon, hysteroscopic fibroid removal is a highly effective, fertility-preserving, and patient-friendly procedure, offering excellent symptom relief with minimal downtime.
Non-Surgical Treatment Options for Fibroids
In very specific clinical scenarios, the following treatments can be considered. However, it is vital to understand how these impact your long-term health and fertility.
1. Uterine Artery Embolisation (UAE):
Uterine artery embolization is a procedure that is performed by an interventional radiologist, and we usually consider it only in very selected situations—most commonly when a patient is not medically fit to undergo surgery and is suffering from significant symptoms like heavy menstrual bleeding.
How It Works:
The procedure involves inserting a fine catheter into an artery, usually through the groin or wrist.
Special particles are released into the uterine arteries to block the blood flow to the fibroid. Without oxygen and nutrition, the fibroid shrinks over time.
The Reality Check:
-
Not a Cure: UAE does not remove the fibroids; it only reduces their size to provide temporary symptomatic relief.
-
Fertility Warning: I do not recommend the UAE for women planning a future pregnancy. It can have a detrimental impact on ovarian reserve (your egg count) and uterine health.
Expert Advice: If you are considering the UAE, I strongly advise taking multiple opinions from both a fibroid specialist and a fertility-focused gynecologist.
2. MRI-Guided Focused Ultrasound (MRgFUS)
A few years ago, this treatment created significant hype as a "non-invasive" miracle. However, in real-world clinical practice, it has largely gone out of vogue.
How it Works: High-intensity ultrasound waves are focused on the fibroid under MRI guidance to generate heat and destroy (lyse) the fibroid tissue.
Why We Exercise Caution:
-
Expensive & Temporary: It is a very costly procedure that often requires multiple sessions but does not offer a permanent solution.
-
Incomplete Results: The fibroid is not removed; it is only partially reduced in volume. In the Indian clinical setting, symptoms often recur.
-
The Gold Standard: When compared to a laparoscopic myomectomy (which completely removes the fibroid), MRgFUS is rarely a logical or cost-effective choice for someone seeking a definitive, fertility-preserving solution.
3. Percutaneous Microwave Ablation (PMWA)
Percutaneous microwave ablation is a relatively newer, minimally invasive technique used to treat fibroids without traditional surgery.
How it Works: A thin needle-like antenna is inserted through the skin (percutaneously) and into the fibroid, usually under ultrasound or CT guidance.
The Reality: Similar to other heat-based treatments, the fibroid remains in the body and is gradually absorbed or scarred down. While it offers a fast recovery, it is generally not recommended for women who wish to conceive, as the effect of high-heat energy on the surrounding uterine environment and future pregnancy outcomes is not yet fully established.
4. Medical (Tablet-Based) Treatment
Medications are frequently used in clinical practice, but it is a common misconception that they "cure" fibroids.
-
Temporary Symptom Control: Tablets (such as GnRH agonists/antagonists, progestins, or tranexamic acid) are primarily used as a temporary measure. They are excellent for controlling heavy menstrual bleeding and reducing pain in the short term.
-
Pre-Surgical Prep: We often use medical therapy to shrink a fibroid slightly or improve a patient's hemoglobin levels before a planned surgery.
-
The Limitation: Once the medication is stopped, the fibroids almost always return to their original size. Therefore, medical therapy is not a permanent solution for removing the growth or permanently restoring fertility.
Consult a Fibroid & Fertility Specialist in Mumbai, India
Before opting for any treatment that sounds "high-tech" or "non-surgical," ask yourself: Does this actually cure the problem, or is it just an expensive temporary fix?
Dr. Jay Mehta and the team at Shree IVF Clinic specialise in fertility-preserving fibroid treatment, with a clear focus on protecting your long-term reproductive health and future fertility.
Take the next step toward the right, targeted solution by booking a priority consultation with Dr. Jay Mehta at our Mumbai fibroid clinic. Call 1800-268-4000 to schedule a comprehensive evaluation and personalised treatment plan
Hormonal Treatment for Fibroids
Many women who experience heavy menstrual bleeding due to fibroids are advised to try hormonal treatments, such as oral contraceptive pills or other hormone-based medications. These treatments can help control bleeding and may provide temporary relief, especially in the short term.
However, it’s important to clearly understand that hormonal treatment does not treat the fibroid itself. It only manages the symptoms. When used as a substitute for surgery, the benefit is usually temporary, and symptoms often return once the medication is stopped.
I often explain this to my patients in simple terms—rather than repeatedly controlling bleeding caused by a fibroid, it may be more effective, when symptoms are present, to treat the root cause by removing the fibroid itself. For symptomatic fibroids, surgical removal is generally considered the most definitive and effective treatment.
That said, every woman is different. The decision between hormonal treatment, surgery, or observation should be made carefully and thoughtfully, after a detailed discussion with a fibroid specialist. Factors such as symptoms, age, future fertility plans, and overall health all matter.
As Dr. Jay Mehta, my focus is always on guiding patients toward a solution that offers long-term relief, not just a temporary fix—while ensuring the choice is right for you.
If you’ve been advised hormonal treatment and feel unsure, a specialist consultation can help you decide the most appropriate and safe next step.
Can Fibroids Shrink with Medication?
Yes—fibroids can shrink with medication, but it’s very important to understand this clearly and honestly.
With hormonal or medical treatment, we do see a temporary reduction in fibroid size, usually around 10–15% after about three months of therapy. This shrinkage can sometimes help reduce symptoms like heavy bleeding or pain while the medication is being taken.
However, there is an important point that many women are not told.
As soon as the medication is stopped, the fibroid usually returns to its original size—often within 2 to 3 weeks.
This means that medical or hormonal treatment does not cure fibroids. It only offers short-term symptom control. Unfortunately, many women are given these medicines with the promise that their fibroids will be “treated” or “eliminated,” which is not scientifically correct.
Similar claims are sometimes made in alternative systems of medicine as well. I strongly advise patients to be cautious with any treatment that promises a permanent cure without surgery.
If someone makes such a claim, it’s reasonable to ask for written evidence and to seek a second opinion from a fibroid specialist.
In my practice, we see many women who come to us after months or years of temporary treatments, only to later discover that the fibroid never truly went away.
Once they understand that medications are temporary and see the scientific data, things often become much clearer.
As Dr. Jay Mehta, I want to be very transparent with my patients: the word “cure” for fibroids can only be used when the fibroid is completely removed, the uterus is carefully reconstructed, and the fibroid bed has healed properly. That is what provides long-term relief and protects future reproductive health.
Key takeaway: Medicines can shrink fibroids temporarily—but they do not cure them. If you’re being advised long-term medical treatment, make sure you fully understand its limitations and consider speaking with a specialist before deciding.
If you’re unsure about your current treatment or have been promised a permanent solution with medication alone, a specialist consultation can help you make a confident, informed decision.
Role of GnRH Analogues in Fibroid Treatment
GnRH analogues—commonly known in India by brand names such as Leupride or Zoladex—are sometimes used in fibroid management, and I like to explain their role very clearly to my patients.
These injections work by temporarily suppressing hormone production from the brain, which in turn reduces ovarian hormone levels—especially estrogen. Since fibroids depend on estrogen to grow, this temporary hormone suppression causes the fibroid to shrink for a short period of time.
However, it’s very important to understand that this effect is completely temporary. Once the effect of the injection wears off, the fibroid usually returns to its original size—often within 2 to 3 weeks. Because of this, GnRH injections do not cure fibroids.
In my practice, I use GnRH analogues only as a short-term measure, most commonly when a patient needs a brief window of 2–3 months to postpone surgery due to personal or medical reasons. They are not meant for long-term treatment.
There was an older belief that taking these injections could make surgery more difficult by disturbing surgical planes.
Based on my experience—and having performed many laparoscopic surgeries after GnRH injections—I can confidently say that this concern is unfounded. These injections do not negatively affect the ease of surgery or the final outcome when performed by an experienced fibroid specialist.
Because of their side effects and temporary nature, GnRH injections are usually given for a maximum of three months and only in carefully selected situations.
As Dr. Jay Mehta, my focus is always on clarity and safety. GnRH analogues can be helpful when used correctly—but they should never be mistaken for a permanent solution. Understanding their limitations helps patients make informed, confident decisions about their care.
Key takeaway: GnRH injections can temporarily shrink fibroids, but they are meant only as a short-term bridge—not a cure.
If you’ve been advised to get these injections and want to understand whether they’re truly appropriate for you, a detailed consultation can help guide the next best step.
Side Effects of Medical Treatment for Fibroids
While medicines for fibroids are often considered because they appear non-invasive, it’s very important for patients to clearly understand their limitations and side effects.
Apart from the fact that medical treatment is usually temporary, many of these oral medications are associated with significant side effects.
Commonly, I see patients experiencing mood swings, emotional changes, and, in some cases, an impact on liver enzymes, which requires close monitoring. Certain medications may also lead to hair fall, and this is one of the most frequent reasons why patients discontinue treatment midway.
Because of these issues, there must be a strong medical indication before starting such drugs. Even then, the maximum duration for which most of these medicines can be safely used is usually 3 to 6 months. And despite completing this course, the reality is that the fibroid itself is not cured.
This is why I strongly encourage patients to consult a fibroid specialist before starting any form of medical management—especially when it is being offered as a “solution” rather than what it truly is: temporary symptom control without long-term benefit.
Limitations of Medicines in Fibroid Treatment
I completely understand why most patients prefer medicines. Surgery naturally feels intimidating, and as humans, we all look for shortcuts or less invasive options.
However, fibroids are one condition where surgical removal of the fibroid remains the treatment of choice, especially when symptoms are present.
Surgery offers two crucial benefits:
- Long-term relief from symptoms
- Protection of future reproductive outcomes, when performed correctly by a specialist
Medical management has a very limited role. It is meant only for temporary use, typically for 3 to 6 months, in patients who need to postpone surgery for personal or medical reasons or, in select cases, to achieve a short-term reduction in fibroid volume.
Even this volume reduction is unpredictable and often does not occur at all when fibroids are larger, particularly those above 8 to 10 cm, which are unfortunately very common in clinical practice.
In India, I frequently see young women being placed on long-term medications with the promise that fibroids will be “cured.” This is scientifically incorrect.
Unfortunately, aggressive marketing, influencer-based social media campaigns, and misinformation make it easy for patients—especially young girls—to fall into this trap.
My strong recommendation is always this: Follow scientific protocols. Seek expert opinion. Consult a fibroid specialist.
Only then should a treatment decision be made—one that is genuinely in the best long-term interest of the patient, not just a temporary compromise.
As Dr. Jay Mehta, my goal is to help patients make informed, safe, and future-focused decisions, rather than quick choices that may delay the right treatment.
What to Expect from Minimally Invasive Fibroid Surgery
For most women with intramural fibroids (fibroids located within the muscular wall of the uterus), minimally invasive surgery is the gold standard. Whether performed via laparoscopy or robotic surgery, these techniques allow for the precise removal of the fibroid while minimizing trauma to the rest of the body.
The Importance of Surgical Expertise
While the removal of the fibroid is the first step, the most critical part of the surgery is the reconstruction of the uterus. Because the fibroid was embedded in the uterine wall, it leaves behind a "space" that must be meticulously sutured.
At Shree IVF Clinic, we emphasize high-level suturing techniques to ensure:
-
Structural Integrity: The uterine wall must be strong enough to stretch and support a growing baby.
-
Minimal Scarring: Reducing the risk of future adhesions that could interfere with fertility.
-
Fast Recovery: Smaller incisions mean less postoperative pain and a quicker return to your daily routine.
Your Roadmap to Recovery and Pregnancy
One of the most common questions we receive is, "How soon can I get pregnant?"
While you will feel back to normal within a week or two, the internal healing of the uterine muscle takes longer.
After surgery, we usually recommend waiting 4–6 months before trying to conceive. This "healing window" is vital to ensure that the uterine scar is robust enough to handle the demands of pregnancy and labor.
Which Fibroid Treatment Preserves the Uterus?
This is one of the most common—and most important—questions I’m asked in my clinic.
The reassuring news is that almost all modern fibroid treatments, when performed by an experienced fibroid specialist, are designed to preserve the uterus. And for the vast majority of women, uterine preservation is exactly what we aim for.
Procedures like myomectomy (fibroid removal)—whether done laparoscopically, robotically, or hysteroscopically—allow us to remove the fibroid completely while keeping the uterus intact. When done correctly, these surgeries also protect and often improve future fertility.
That said, there are rare situations where a woman has:
- Multiple fibroids
- Repeated recurrences despite prior surgeries
- Severe symptoms that significantly affect quality of life
In such cases, hysterectomy may be discussed as an option, but it is never a first-line recommendation. It is always a shared decision, taken only after detailed counseling and careful consideration of the woman’s age, symptoms, and future plans.
What truly makes the difference here is. Even in complex cases with multiple fibroids, a dedicated fibroid specialist can often preserve the uterus and ensure excellent long-term reproductive outcomes. That is why I strongly encourage women to seek care at a centre that routinely manages complex fibroid cases.
Which Treatment Is Best for Large Fibroids?
When it comes to large fibroids, clarity is essential.
The best and most effective treatment for a large fibroid is complete surgical removal—especially when the surgery is performed by a specialist who focuses on fibroid management and minimally invasive techniques.
Large fibroids can sit in challenging locations and may distort the uterus or press on nearby organs. This is why careful pre-surgical planning and detailed fibroid mapping are critical before treatment. When done properly, removing a large fibroid can actually improve fertility and relieve long-standing symptoms.
With today’s advances in minimally invasive and robotic surgery, even very large fibroids can be removed safely through small incisions. The benefits include:
- Faster recovery
- Minimal scarring
- Less pain
- Excellent cosmetic results
Most importantly, the uterus is reconstructed meticulously, preserving its strength and function for the future.
A helpful tip: Large fibroids should not be ignored—but they also don’t mean you’ll lose your uterus. With the right expertise, the outcomes can be excellent.
If you’ve been told you have large or multiple fibroids, make sure you discuss your options with a specialist who routinely performs advanced fibroid surgery and prioritises uterine preservation.
How to decide between myomectomy and hysterectomy?
This is a very important decision, and I always tell my patients that it should never be rushed.
In simple terms, a hysterectomy (removal of the uterus) should be considered only in very specific situations—typically when a woman has completed her family, has multiple or recurrent fibroids, and is very clear that she no longer wishes to preserve her uterus.
For every other woman diagnosed with fibroids, especially those in the reproductive age group, the focus should strongly be on uterus-conserving surgery, which is a myomectomy.
In fact, for most women, myomectomy is the treatment of choice because it removes the disease while preserving the uterus and future reproductive potential.
I also want to clarify one common misconception. Temporary or noninvasive treatments—whether hormonal medicines, injections, or other modalities—do not cure fibroids.
These options are reserved only for patients who are temporarily unfit for surgery or who need a short window to postpone surgery for medical or personal reasons. They should never replace definitive treatment in a woman who is otherwise fit for surgery.
The decision between a myomectomy and a hysterectomy must always be made after:
- Understanding your age and fertility goals
- Assessing the number, size, and location of fibroids
- Evaluating symptoms and recurrence risk
- Having a detailed discussion with a fibroid specialist
When this decision is taken with the right guidance, it ensures that the treatment chosen is truly in the best interest of your long-term health and quality of life.
Is uterus-saving fibroid treatment possible?
Yes—absolutely. And this is one of the most common concerns I hear from my patients.
The majority of women diagnosed with fibroids are in their reproductive years, and for them, saving the uterus is a top priority.
I want to reassure you that in most situations where fibroid removal is required, uterus-preserving surgery is very much possible.
Today, fibroid surgery is largely performed using laparoscopic or robotic techniques, and when done by an experienced fibroid specialist, uterine conservation is the default goal, not the exception.
During a myomectomy, we carefully remove only the fibroid, reconstruct the uterus layer by layer, and ensure optimal healing—so that fertility potential is not just preserved but often significantly improved.
This is precisely why choosing a fibroid specialist matters. Expertise allows us to achieve the following:
- Complete disease clearance
- Minimal blood loss
- Strong uterine reconstruction
- Excellent future reproductive outcomes
There are, however, a few situations where uterus removal (hysterectomy) may be discussed—typically in women who have recurrent fibroids or multiple fibroids when the family is already complete. Even then, this decision is never rushed and is taken only after detailed counselling and shared decision-making.
My message to every woman is simple:
Uterus-saving fibroid treatment is not only possible, it is routinely done—when managed by the right specialist, for the right patient, at the right time. - Dr. Jay Mehta
Is Surgery Always Needed for Fibroids?
Not all fibroids require surgery. The need for treatment depends on several factors, including the number, size, and location of the fibroids. For example:
- A small submucous fibroid (1 cm) that grows inside the uterus may need surgical removal.
- A larger subserosal fibroid (4 cm) on the outer surface of the uterus may not cause any symptoms and often does not require immediate treatment.
Fibroid management is highly personalized, and the best approach depends on your individual situation, symptoms, and future plans.
Next step: Book a consultation with an experienced gynecologist and fibroid specialist to evaluate your condition and discuss the most suitable treatment options for you.
How to Approach Fibroid Management?
Fibroid care is personalized. The right approach depends on your symptoms, the size and location of the fibroids, and your personal preferences.
Regular monitoring and guidance from an experienced specialist are essential for making the best decisions about your health.
Always talk openly with a fibroid specialist to understand all your options. Early evaluation and expert advice can help prevent complications in the future. Fibroid management can be complex and differs from person to person.
Dr. Jay Mehta, with his expertise in fibroid care and gynecology in Mumbai, can help create a treatment plan tailored specifically to you.
Don’t hesitate to seek professional advice—it ensures peace of mind and the best possible care.
Will Fibroid Surgery Affect Future Childbirth?
This is a very common concern. In most cases, fibroid surgery does not automatically mean a C-section in the future.
A common concern is whether fibroid removal surgery necessitates a Cesarean section for future births. This is generally not the case.
As long as the uterus is repaired skillfully, the method of fibroid removal (whether the incision is transverse, horizontal, or elliptical) does not dictate the need for a C-section. The most critical factor is the quality of the uterine repair, ensuring the "dead space" is closed with sutures for optimal healing.
During surgery, we prefer to temporarily reduce blood flow to the uterus instead of using drugs like vasopressin, which can have cardiac side effects. This technique minimizes blood loss and enhances safety.
Fibroids are common—but their treatment should always be personalized.
If you’re dealing with multiple fibroids, symptoms, or fertility concerns, a specialist evaluation can bring clarity and peace of mind.
Schedule a consultation with Dr. Jay Mehta to discuss advanced, minimally invasive fibroid care that protects your health and your future.
What Happens If Fibroids Are Untreated?
In the vast majority of cases, nothing serious happens—especially when fibroids are small and completely asymptomatic.
When I diagnose a small fibroid that is not causing any symptoms, I usually do not recommend any treatment at all. In fact, in more than 80% of such situations, fibroids either remain stable in size or grow so slowly that they never become a problem.
What I do recommend is an annual follow-up. This allows us to:
- Track the exact size and location of the fibroid through fibroid mapping
- Compare serial measurements over time
- Decide calmly and rationally only if and when treatment is truly needed
Over the last 12–13 years of my clinical practice, I have seen countless women who were advised not to undergo surgery because their fibroids were small—and the vast majority of them never required surgery later either.
Fibroids are not an emergency disease. They are a slow, benign condition, and most women live their entire lives without any complications from them.
The key, however, is being a responsible and informed patient:
- Stick to regular follow-ups
- Report any new symptoms early
- Stay connected with your fibroid specialist
If you are willing to do that, fibroids can usually be managed very comfortably, and your journey with this condition can be smooth, safe, and stress-free.
Can Fibroids Recur After Treatment?
Yes, fibroids can recur after treatment, and this is something I always discuss very clearly with my patients before we plan any surgery.
If a woman has a single (solitary) fibroid, the risk of recurrence is extremely low—less than 1%. Of course, this also depends on how meticulously the first surgery is performed and the experience of the fibroid specialist handling the case.
When there are multiple fibroids, the chances of recurrence gradually increase:
- If there are more than 5 fibroids, the recurrence risk is around 5–8%
- If there are more than 10 fibroids, the risk rises to over 10%
- And when there are 15–20 fibroids, the recurrence risk can be as high as 20–25%
This information is a mandatory part of my presurgical counselling.
I strongly believe in being completely honest with my patients, because this transparency helps them make wise and informed decisions, especially regarding their future fertility plans.
It is very important to understand that no surgical treatment in the world can guarantee a 0% recurrence rate for fibroids. Surgery treats the existing fibroids—it does not change the underlying tendency of the uterus to form new ones.
That is why, if recurrence risk and fertility planning are major concerns for you, I always advise patients to consider a second opinion from a fertility specialist before proceeding with surgery. The goal is not just successful surgery but long-term reproductive and overall health.
Informed decisions lead to better outcomes—and that is always my priority for my patients.
When Should Fibroids Be Treated Urgently?
In the majority of cases, fibroid surgery is not an emergency and can be planned electively after proper evaluation and counselling. However, there are a few exceptional situations where urgent or emergency intervention becomes necessary.
Urgent treatment is required in the following scenarios:
- Torsion of a fibroid
When a pedunculated fibroid twists on its stalk, it can cause sudden, severe abdominal pain and compromised blood supply. This situation often warrants emergency surgery.
- Torrential bleeding from a submucous fibroid
Submucous fibroids can sometimes lead to profuse, uncontrollable uterine bleeding, which may not respond to medical management. In such cases, urgent surgical intervention becomes mandatory.
- Severe anaemia due to heavy menstrual bleeding
Fibroids associated with chronic heavy menstrual bleeding can result in significant anemia. If the haemoglobin levels drop to dangerous levels, the patient may require:
-
- Urgent hospital admission
- Correction of anaemia (iron therapy or blood transfusion, if needed)
- Definitive surgical management once the patient is stabilised
In summary, while fibroid surgery is usually planned and non-emergent, acute pain, excessive bleeding, or severe anaemia are red flags that should never be ignored. Prompt medical attention in these situations can be life-saving and fertility-preserving.
Severe Bleeding Due to Fibroids – When Should You Worry?
As a fibroid specialist, I often tell my patients that not all bleeding is dangerous, but certain patterns of bleeding should never be ignored.
Severe bleeding related to fibroids is most commonly seen in:
- Large submucous fibroids, or
- Large intramural fibroids that significantly distort the endometrial cavity, which is the inner lining of the uterus.
Now, how do you know when bleeding is crossing the line from “manageable” to “concerning”?
A clear warning sign is when:
- You are using more than four sanitary pads per day.
- For more than four days during a single menstrual cycle.
When bleeding reaches this level, it is no longer considered normal menstrual flow. At this point, I strongly advise patients to consult a fibroid specialist without delay.
Why is this important? Because persistent heavy bleeding can rapidly deplete your iron stores, leading to anaemia, fatigue, breathlessness, and a significant drop in overall quality of life. If ignored, this can eventually land a patient in an emergency situation.
In such cases, a detailed evaluation—including imaging and fibroid mapping—is essential. Very often, this degree of bleeding becomes a strong indication for timely surgical management, not as a matter of urgency alone, but to protect your long-term health and well-being.
My advice is simple:
If your periods are becoming heavier, longer, or more exhausting with each cycle, don’t normalize it, and don’t wait it out. Early intervention can prevent major complications and make your treatment journey much smoother.
Rapidly Growing Fibroid – Is It Dangerous?
This is a very important question, and I’m glad you’re asking it.
In my practice, I strongly encourage every woman who has a fibroid—even if it is small and asymptomatic—to have at least one follow-up every year with a fibroid specialist.
Ideally, this follow-up should be done using a fibroid-mapping ultrasound, which is a specialised scan that accurately tracks the exact size, number, and location of fibroids over time.
Now, coming to the concern about rapid growth.
Most fibroids grow very slowly, or sometimes they don’t grow at all. However, if a fibroid increases very rapidly in size—especially if it more than doubles within a single year—this becomes a red-flag sign.
Such rapid growth is uncommon, but when it does happen, it raises a concern that the fibroid may not be behaving in a benign manner. In rare situations, this can indicate a possibility of a cancerous change, and this warning sign should never be ignored.
This is precisely why I insist on regular annual follow-ups, particularly for women who are currently not keen on surgery. Timely monitoring allows us to:
- Detect abnormal growth early
- Take the right decision at the right time
- Avoid delays or emergencies
My reassurance to you is this: most fibroids are completely benign. But my responsibility as your doctor is to make sure that nothing dangerous is missed. Regular follow-up is not about creating fear—it’s about ensuring safety, clarity, and peace of mind.
If you’re living with a fibroid and choosing observation, make sure it’s active observation, guided by a specialist. That one step can make all the difference in your long-term health journey.
Fibroids Causing Severe Anemia
This is something I see very commonly in day-to-day practice, especially in India.
Fibroids that are associated with heavy menstrual bleeding are the main culprits when it comes to anemia. In particular, submucous fibroids, or intramural fibroids that distort the endometrial cavity (the inner lining of the uterus), tend to cause excessive and prolonged periods.
When this heavy bleeding continues month after month, it can gradually lead to severe iron-deficiency anemia.
Interestingly, many times the first diagnosis is actually anemia, and the fibroid is discovered only later.
In a country like India, where anemia is already very common across all age groups and social backgrounds, fibroids often go unnoticed until the hemoglobin drops significantly and the patient starts feeling symptoms like fatigue, breathlessness, dizziness, or palpitations.
From a treatment point of view, my approach is very clear and patient-centric.
In the majority of cases, we first correct the anemia—either with oral iron therapy, intravenous iron, or blood transfusion if required—before proceeding with surgical management of the fibroid. This makes the surgery much safer and helps the patient recover faster.
The key message I always give my patients is this:
If heavy periods are being ignored, anemia can quietly worsen. Treating the fibroid at the right time not only controls the bleeding but also restores overall health and quality of life. Early evaluation and timely intervention make a huge difference.
Fibroids with Severe Pain
Fibroids associated with severe pelvic pain are most commonly submucous fibroids or large intramural fibroids.
In many patients, this pain is not due to fibroids alone. Quite often, fibroids coexist with endometriosis, and these two conditions frequently go hand in hand. When present together, they can cause intense and persistent pelvic pain, significantly affecting a woman’s quality of life.
In such situations, a thorough pelvic evaluation is essential. This should ideally include fibroid mapping to accurately identify the size, number, and location of fibroids, along with endometriosis mapping (endo-mapping) to assess the extent and depth of endometriotic involvement in the pelvis.
This detailed evaluation helps in understanding the true nature of the disease and in planning the most effective treatment strategy.
When fibroids are associated with severe pain, surgical management is usually the treatment of choice for most patients.
Medical management in these cases is often ineffective or provides only minimal and temporary relief. Delaying definitive treatment by repeatedly trying medical therapy may unnecessarily prolong the patient’s suffering.
Therefore, women experiencing severe pain due to fibroids should seek timely consultation with a fibroid and endometriosis specialist.
Early surgical intervention, when appropriately planned and performed using minimally invasive techniques, can provide significant and long-lasting relief while preserving pelvic health and fertility wherever possible.
Can fibroids disappear naturally?
This is a very common question I hear in my clinic, and I like to answer it very honestly and simply.
Fibroids do not disappear on their own. Once a fibroid has been correctly diagnosed, it does not magically vanish. Even after menopause—when hormonal support reduces—fibroids may shrink in size, but they do not disappear completely.
So, if someone has been told that their fibroid has “completely disappeared,” there is a strong possibility that it may not have been a fibroid to begin with or that the initial diagnosis was incorrect.
Menopause can certainly make fibroids quieter and smaller because estrogen support is withdrawn, but the fibroid tissue itself usually remains, sometimes undergoing changes like calcification rather than vanishing altogether.
This is why I strongly recommend proper imaging, accurate diagnosis, and periodic follow-up with a fibroid specialist.
Clear facts help avoid unnecessary anxiety, false reassurance, or misinformation—especially when advice is picked up from social media or non-medical sources.
The key takeaway I always tell my patients is this: Fibroids can shrink, and they can become inactive, but they do not truly disappear naturally.
Can fibroids be cured by diet?
This is a very common question I hear in my clinic, and I completely understand why patients ask this.
To be very clear and honest with you—as of today, there is no scientifically proven diet that can cure fibroids or make them disappear. There is no medical evidence to show that any specific food, supplement, or dietary plan can permanently shrink or eliminate fibroids.
Now, if you search online, you will find numerous claims—special diets, detox plans, herbal remedies, or paid programs that promise to reduce fibroid size or cure fibroids naturally. I would urge you to be extremely cautious with such claims. Most of these are not backed by strong scientific data, and many patients end up spending a lot of money without real benefit.
That said, a healthy, balanced diet does play a role in overall well-being. Good nutrition can help:
- Improve energy levels
- Support correction of anemia
- Reduce inflammation
- Help you cope better with symptoms
But diet alone cannot replace proper medical or surgical treatment when fibroids are symptomatic or large.
My sincere advice to every patient is this: do not fall prey to false promises. Before starting any special diet, supplement, or paid therapy, please discuss it with your doctor or a fibroid specialist. Making informed decisions will always protect your health—and your peace of mind.
As your doctor, my goal is always to guide you with facts, not fear or false hope.
Do Alternative Therapies Work for Fibroids?
Many patients ask whether treatments like Ayurveda, homeopathy, or specialized diets can cure fibroids.
As a specialist who manages these cases daily, I want to answer this in a transparent, honest, and patient-friendly manner.
The Scientific Reality of Alternative Medicine
It is important to be clear: Speaking purely from clinical experience and evidence-based medicine, there is currently no alternative therapy that can permanently cure or "dissolve" fibroids.
A fibroid is a structural, muscular growth within the uterus. Once these growths have formed, they cannot be reversed or eliminated by tablets, herbs, diets, or lifestyle changes alone.
While patients are often drawn to alternative medicine because it is perceived as "natural," any substance that has a physiological effect on the body can also have side effects, especially when taken over long durations without proper monitoring.
The Role of Complementary Care
While they cannot shrink or eliminate the actual growth, some patients feel that alternative therapies provide value in other ways:
- General Well-being: Supporting overall physical and mental health.
- Symptom Control: Assisting with minor pain or inflammation management.
- Recurrence Support: Potentially supporting the body after a definitive medical or surgical treatment has already been performed.
⚠️ A Crucial Clinical Warning
The biggest risk of relying solely on alternative cures is the loss of valuable time.
I often see manageable fibroids grow into "massive," bulky uterine masses because a patient delayed specialist care in the hope that an alternative treatment would work.
This delay can make future surgery more complex, and, more importantly, it can significantly impact the ovarian reserve and fertility of women planning a pregnancy.
Expert Tip: Balanced and Respectful Advice
My advice to you is simple and heartfelt:
- Seek Clarity: Be cautious of anyone promising to "cure" fibroids without surgery or proven medical treatment.
- Complement, Don't Replace: You are free to explore complementary approaches for general symptom relief, but they should never replace evidence-based medical evaluation.
- Don't Delay: Do not postpone a specialist consultation if you have worsening symptoms or are planning to conceive.
Dr. Jay Mehta’s Perspective: A well-informed decision, guided by facts rather than false promises, will always be the best way to protect your long-term health and fertility.
The only definitive and permanent treatment for a symptomatic fibroid remains surgical removal, ideally performed through minimally invasive techniques.
If alternative therapies haven’t brought you relief or your symptoms are getting worse, it may be time for a specialist evaluation.
Schedule a consultation with Dr. Jay Mehta at Shree IVF Clinic, Mumbai, for a clear diagnosis and a personalised treatment plan.
📞 Call 1800-268-4000 to book your appointment, or opt for an online consultation if you’re outside Mumbai—where Dr. Jay Mehta can assess your reports and guide you with a transparent, step-by-step clinical roadmap.
Do fibroids always need surgery?
This is one of the most reassuring conversations I have with my patients—and the answer is no, fibroids do not always need surgery.
In fact, the majority of fibroids we diagnose are tiny, seedling fibroids.
These are very common and, in most situations, do not require any surgical treatment at all.
For such fibroids, I usually recommend a simple annual follow-up. This helps us keep an eye on their size and location and gives both the patient and me long-term clarity and peace of mind.
Surgery becomes a consideration only in specific situations. Fibroids that cause symptoms, such as heavy bleeding or pain, or fibroids that affect fertility or reproductive outcomes, often leave us with no effective alternative to surgical removal.
In these cases, surgery is not about urgency—it’s about improving quality of life and future reproductive potential.
On the other hand, small fibroids that are not distorting the endometrial cavity and are not affecting fertility can safely be observed.
Many women live comfortably for years with such fibroids without any progression or complications.
There are, however, situations where I advise surgery even if symptoms are minimal. Very large fibroids—typically more than 6 to 7 cm in size—often warrant removal, even if they are not currently causing problems.
This is because large fibroids can create future complications and make surgery more complex if delayed.
When surgery is required, it is almost always performed using minimally invasive techniques, such as laparoscopic or robotic surgery, which allow for faster recovery, excellent cosmetic results, and preservation of the uterus whenever possible.
My approach is always simple: individualise the decision, avoid unnecessary surgery, and intervene only when it truly benefits the patient’s health, comfort, or fertility.
When should you seek a fibroid specialist?
As a doctor who deals with fibroids daily, I genuinely believe that every woman diagnosed with a fibroid should consult a fibroid specialist at least once.
While fibroids are common, their management is anything but simple. The decision to observe, treat with medication, or perform surgery depends on a complex interplay of your age, symptoms, the fibroid’s location, and—most importantly—your future fertility goals.
Why Specialized Expertise Matters in Fibroide cure
Many women are advised to undergo treatment without a full explanation of their options.
This is why patients from across India seek online consultations with us, especially when surgery has been suggested. They aren't just looking for a second opinion; they are looking for clarity and reassurance.
-
Experience Over Proximity: In India, it is natural to visit the doctor closest to home. However, because fibroid management is so nuanced, you need a specialist at a center where fertility-preserving surgeries are performed routinely.
-
Reconstruction is key: If surgery is needed, it’s not just about "removing the lump." It is about reconstructing the uterus so that it can heal optimally for a future pregnancy.
-
High-Volume Care: Shree IVF Clinic is one of the very few dedicated fibroid units in India.
We approach fibroid management in a structured, scientific, and patient-centric manner.
How to choose the right fibroid treatment in India?
This is a very important question, and I’m glad you’re asking it.
In a country like India, most people naturally tend to visit the doctor who is closest to their home. That doctor may be very good but may not necessarily be a dedicated fibroid specialist.
Fibroid management today is highly nuanced and depends on multiple factors such as the size, number, and location of fibroids; symptoms; fertility goals; and future reproductive planning. This is exactly where specialised expertise becomes critical.
A specialist like Dr. Jay Mehta, one of the top fibroid surgeons in Mumbai, India, focuses on personalized treatment rather than a "one-size-fits-all" approach.
Why Expertise Matters
- Avoid Unnecessary Procedures: Seek an opinion from a center where fertility-preserving, minimally invasive techniques are performed routinely.
- Specialized Units: There are very few dedicated fibroid units in India. Shree IVF Clinic is a leading center where fibroid management is structured, scientific, and patient-centric.
- Global Access: We consult patients across India and internationally via online consultations, helping them gain clarity and avoid temporary treatments before they travel to Mumbai for care.
These consultations help patients gain clarity, avoid unnecessary or temporary treatments, and make informed decisions that are truly in their best long-term interest.
Choosing the right fibroid treatment is not about rushing into surgery or blindly opting for medical therapy—it is about personalised decision-making, guided by a specialist who understands fibroids, fertility, and minimally invasive surgery in depth.
And that decision is best made at a centre like Shree IVF Clinic, where comprehensive fibroid care is routinely practiced.
Fibroid Treatment Success Stories (Patient Case Studies) at Shree IVF Clinic
Real patient outcomes help women understand how fibroid treatment can improve both health and fertility outcomes. At our center, many patients with complex fibroids have successfully preserved their uterus and achieved pregnancy after treatment.
Case Study: Successful Pregnancy After Fibroid Removal
Patient Age: 34 years
Condition: Large fibroid causing infertility and repeated IVF failure
The patient had a 9 cm intramural fibroid affecting the uterine cavity, which was interfering with embryo implantation and contributing to repeated IVF failure.
She had previously been advised to undergo a hysterectomy at another center because of the fibroid’s size and location.
After a detailed evaluation by Dr. Jay Mehta, a fertility-preserving laparoscopic myomectomy in Mumbai was recommended.
The goal was to safely remove the fibroid while preserving the uterus and improving the chances of pregnancy.
Treatment Approach
A minimally invasive laparoscopic fibroid surgery was performed to remove the large fibroid with precision while reconstructing the uterine wall carefully to maintain uterine strength for future pregnancy.
Outcome
- Fibroid successfully removed
- Uterus preserved with proper uterine reconstruction
- IVF treatment performed later
- The patient achieved a successful pregnancy
This case highlights how advanced fibroid treatment in India can help women preserve fertility even in complex cases that were previously considered suitable only for hysterectomy.
Case Study: Recurrent Fibroid after Previous Surgery
Patient Age: 36 years
Condition: Recurrence of fibroids after previous surgery affecting fertility
The patient had previously undergone fibroid surgery at another center but later developed recurrent uterine fibroids, which began affecting her fertility and chances of conception.
Seeking a second opinion, she consulted Dr. Jay Mehta for further evaluation. After a detailed assessment, a specialized fertility-preserving surgical approach was planned to safely remove the recurrent fibroids while maintaining the strength and structure of the uterus.
Treatment Approach
A carefully planned minimally invasive fibroid removal surgery in Mumbai was performed to remove the recurrent fibroids. During the procedure, special attention was given to reconstructing the uterine wall, ensuring that the uterus remained strong enough to support future pregnancy.
Outcome
- Recurrent fibroids successfully removed
- Uterine structure preserved
- Patient can pursue fertility treatment
This case demonstrates how advanced fibroid treatment in India can successfully manage recurrent fibroids, helping women preserve fertility and continue their journey toward pregnancy.
Why Choose Dr. Jay Mehta for Fibroid Treatment in Mumbai, India
When dealing with uterine fibroids, choosing the right fibroid specialist in India can make a major difference in treatment outcomes—especially for women who wish to preserve their uterus and future fertility.
Dr. Jay Mehta is recognized internationally for managing complex and previously untreated fibroid cases. Patients looking for the best doctors for uterine fibroid treatment and the best hospitals for fibroid surgery in India often consult him for expert evaluation and advanced treatment options.
His approach combines advanced minimally invasive fibroid surgery in Mumbai with fertility-focused treatment planning.
Below are the key reasons patients from Mumbai, across India, and international countries choose Dr. Mehta for fibroid treatment.
Uterine-Sparing Expertise
One of the primary goals of fibroid treatment is to remove fibroids while preserving the uterus whenever possible.
Dr. Mehta is highly experienced in performing fertility-preserving myomectomy, including cases where patients were previously advised to undergo hysterectomy.
Many women with large, multiple, or complex fibroids have successfully preserved their uterus through advanced surgical techniques designed to remove fibroids safely while maintaining uterine strength.
Advanced Minimally Invasive Technology
Dr. Mehta utilizes modern surgical platforms such as laparoscopic and robotic techniques, which provide greater precision and faster recovery compared to traditional open surgery.
Benefits of minimally invasive fibroid surgery include:
- Smaller surgical incisions
- Minimal blood loss
- Reduced hospital stay
- Faster recovery time
- Less post-operative discomfort
- Minimal scarring
This approach allows many patients to return to normal activities sooner.
Fertility-Focused Treatment Approach
As both a fertility specialist and gynecological surgeon in Mumbai, Dr. Mehta takes a fertility-first approach when treating fibroids.
Special surgical suturing techniques are used to ensure that:
- The uterine wall heals properly
- The uterus remains strong enough to support a future pregnancy
- The risk of complications during pregnancy is minimized
This integrated approach is particularly beneficial for women who are planning pregnancy after fibroid treatment.
Proven Track Record in Complex Cases
Dr. Mehta has treated thousands of patients with fibroids, including challenging cases that require highly specialized surgical planning.
His experience includes:
- Treating large fibroids
- Managing multiple fibroids
- Performing repeat fibroid surgeries
- Treating fibroids affecting fertility
Because of this expertise, many women searching for a fibroid specialist in India seek a second opinion from Dr. Mehta before undergoing a hysterectomy.
Trusted by Patients Across India and Internationally
Patients travel from across India and internationally to seek treatment with Dr. Mehta due to his experience in advanced fibroid surgery and fertility preservation.
The clinic offers support for:
- Online consultation for distant patients
- Treatment planning before travel
- Assistance for international medical patients
This makes the treatment process smooth and coordinated for patients traveling from outside Mumbai or abroad.
Fibroid Treatment Cost in India
The cost of fibroid treatment in India can vary depending on several factors, such as the size and number of the fibroids, the type of treatment required, hospital facilities, and the expertise of the treating doctor.
India has become a preferred destination for fibroid treatment because patients receive advanced gynecological care at affordable costs compared to many countries.
Average Cost of Fibroid Treatment in India
| Treatment Type | Average Cost Range |
|---|---|
| Consultation & Diagnosis | ₹2,500 – ₹7,000 |
| Medical Management (Hormonal Medicines) | ₹6,000 – ₹30,000 |
| Myomectomy (Fibroid Removal Surgery) | ₹1,20,000 – ₹2,50,000 |
| Laparoscopic Myomectomy | ₹1,80,000 – ₹3,00,000 |
| Hysteroscopic Fibroid Removal | ₹1,00,000 – ₹2,00,000 |
| Uterine Artery Embolization (UAE) | ₹2,00,000 – ₹3,50,000 |
Note: The costs mentioned for these procedures are estimates and do not represent the exact final cost. Hospital charges may vary based on the choice of room category and facility.
Because fibroid treatment is highly individualized, a definitive financial breakdown can only be provided after a clinical evaluation.
Please consult Dr. Jay Mehta, a leading fibroid specialist in India, or call 1800-268-4000 for accurate pricing tailored to your specific medical needs.
Cost Advantage for International Patients
Many international patients choose India because they receive high-quality fibroid treatment at a fraction of the cost compared to countries like the USA, UK, and Europe, along with access to experienced specialists and modern surgical techniques.
Patients traveling for treatment can also receive assistance with:
- Medical visa guidance
- Airport pickup
- Accommodation support
- Treatment coordination
If you are experiencing symptoms like heavy bleeding, pelvic pain, or fertility issues, consulting a specialist early can help determine the most effective and cost-efficient treatment plan.
Fibroid Treatment Options Comparison
Different fibroid treatments are recommended depending on symptoms, fibroid size, fertility goals, and patient age.
| Treatment Option | Best For | Uterus Preserved | Recovery Time |
|---|---|---|---|
| Medical Management | Mild symptoms, small fibroids | Yes | No surgery |
| Myomectomy | Women planning pregnancy | Yes | 2–4 weeks |
| Laparoscopic Myomectomy | Medium to large fibroids | Yes | 1–2 weeks |
| Hysteroscopic Fibroid Removal | Fibroids inside uterus | Yes | Few days |
| Uterine Artery Embolization | Symptom control | Usually yes | 1–2 weeks |
| Hysterectomy | Severe cases not requiring fertility | No | 4–6 weeks |
Choosing the right treatment requires evaluation by a specialist who can assess:
• Fibroid size
• Fibroid location
• Number of fibroids
• Fertility goals
• Overall reproductive health
An individualized treatment plan ensures the most effective and safest outcome.
Frequently Asked Questions About Uterine Fibroids
- Can fibroids affect fertility?
Yes. Certain types of fibroids—especially submucosal fibroids and large intramural fibroids—can interfere with embryo implantation, increase miscarriage risk, and affect IVF success rates. Proper diagnosis and treatment can significantly improve fertility outcomes.
- Can I get pregnant with fibroids?
Yes, many women with fibroids can still conceive naturally. However, certain fibroids—especially those inside the uterine cavity—can interfere with implantation or increase miscarriage risk. Treatment by an experienced specialist such as Dr. Jay Mehta may improve fertility outcomes.
- When should fibroids be removed?
Fibroid removal may be recommended if you experience Heavy menstrual bleeding, pelvic pain or pelvic pressure, infertility or repeated IVF failure, rapid fibroid growth, or fibroids distorting the uterine cavity. In such cases, consulting an experienced fibroid specialist can help determine the most appropriate treatment plan.
- What is the best treatment for fibroids?
The best treatment depends on several factors, including the size of the fibroid, the location of the fibroid, the number of fibroids, symptoms, and fertility goals. For women planning pregnancy, myomectomy (fibroid removal surgery) is often recommended because it removes fibroids while preserving the uterus.
- Who is the best laparoscopic surgeon in Mumbai, India, for fibroid treatment?
Choosing the best surgeon depends on experience, surgical expertise, and specialization in fertility-preserving procedures. Many women seeking advanced fibroid treatment consult Dr. Jay Mehta because of his experience in minimally invasive fibroid surgery and fertility-focused treatment planning.
- Can fibroids come back after surgery?
Yes, fibroids can recur in some women. However, the risk of recurrence can be reduced with proper surgical technique, complete fibroid removal, and regular follow-up care.
- Is laparoscopic fibroid surgery safe?
Yes, laparoscopic myomectomy is a safe and effective minimally invasive procedure when performed by an experienced surgeon such as Dr. Jay Mehta. Compared to traditional open surgery, this technique offers several benefits like smaller incisions, less blood loss, faster recovery and shorter hospital stay.
- Are there new treatments for fibroids without surgery in India?
Yes. Some non-surgical or minimally invasive treatments for fibroids include hormonal medications to control symptoms, uterine artery embolization (UAE), and MRI-guided focused ultrasound therapy.
However, for women planning pregnancy, myomectomy is often considered the most effective fertility-preserving treatment.

Dr. Jay Mehta
MBBS, DNB—Obstetrics & Gynecology
IVF & Endometriosis Specialist, Laparoscopic Surgeon (Obs & Gyn)

4.9
![]()
Verified & Most Trusted One
Dr. Jay Mehta is a highly renowned IVF specialist and fertility-preserving surgeon based in Mumbai, India. As the director of the Shree IVF and Endometriosis Clinic, Mumbai, he is recognized as one of India's leading laparoscopic gynecologists for the advanced treatment of complex conditions such as endometriosis and adenomyosis.
Dr. Mehta's expertise extends deeply into reproductive medicine; he is a well-known IVF specialist and among the few practitioners in the country with specialized knowledge in embryology, andrology, reproductive immunology, and Mullerian anomalies. Dr. Mehta conducts operations and consultations across India's major cities, including Pune, Chennai, Hyderabad, Bangalore, Ahmedabad, Agra, and Delhi. To book an appointment, call: 1800-268-4000
Many Treatments. One Goal.
Caring for Every Patient, Every Day.
Jyoti Walmiki
In 2017 during pregnacy we got to know that I have large uterine fibroid, I underwent laparoscopic fibroid removal with Dr.Jay Mehta.Its excellent recovery.
Excellent facilities and Excellent staff with affordable charges.
Thanku so much Dr.Jay Mehta.
Aditi Jain
We were referred to Dr Jay Mehta’s clinic by several family doctor friends in Indore for fibroid treatment. They were able take us in with minimum delay and also operate sooner than expected. The facility is very good. The building is currently undergoing construction on the outside so we were a little concerned but out concerns went away as soon as we entered the facility. The staff was also very helpful throughout our time at the hospital. Overall Dr Jay Mehta is very knowledgeable and experienced laparoscopic surgeon and was able to treat us very professionally and expertly. Would recommend to anyone in india and abroad.
Kavita Raikuvar
I had large central fibroid, in report it was showing around 18cm but while operating it was found to be 20 cm which took approx 4.5 hours of surgery by 3D laparoscopy. I was completely in safe hand and good care was taken of mine from getting admitted to discharge that was within 48 hours. Excellent service and good support from staff.
Jitendra Jain
My wife was diagnosed with huge fibroid and her tummy was looking like she is pregnant,which ever doctor we have visited have advised that she have to undergo surgery which will have big cut on her tummy,qfter visiting many doctors we have met Dr jay mehta,who us the only one who told who can operate by laparoscopy,and did it with just 3holes,and to our surprise4hrs after surgery she was walking and got dischargedby night,Doctor is reallydynamic and had great experience wid him
Krupa Sheth
I have been diagnosed with large fibroid to my surprise, I was scared and confused. I want to thank Dr Jay and his team who took care by doing laparoscopy surgery for the fibroid.
Ganga V
Dr. Jay Mehta performed my fibroid surgery; I've never seen a doctor as good as this.
To be honest, he performed open surgery on me on January 11, 2025, at the Bharathi Super Speciality Hospital in Nizamabad. He destroyed my uterus, twisted my large uterine bone, and performed a hysterectomy on the uterus. He didn't even give me a discharge report. The report doesn't say anything; he just says this medicine.
Dr. Jay Mehta Sir clarified my problem and made me eligible to become a mother. Natural pregnancy is difficult due to my previous condition, and the chances of conceiving through IVF are high. Donor eggs are not even a concern here; they use their own eggs. I recommend the best doctor in India, Dr. Jay Mehta.
Blogs

Bulky Uterus & Uterine Fibroids : Understanding Diagnosis, Treatments, Risks & more
In this blog, we’ll detail some of the typical signs and causes associated with both types of fertility issues.
Can Fibroids Cause Urine Leakage?
Urinary incontinence is more prevalent in women than men and can be caused by numerous health conditions such as childbirth or pelvic surgery
Videos

Urinary Incontinence – Symptoms and Causes
Urge incontinence primarily stems from a weakened internal sphincter, which is essentially a muscular valve that controls the release of urine from the bladder

How to treat Overactive bladder?
Urge incontinence is extremely amenable to treatment when treated correctly. There are a lot of medical management options available in order to treat urge incontinence.