India’s 1st Chronic Pelvic Pain & NeuroPelveology Clinic: A New Era in Women’s Healthcare

Advanced Multidisciplinary Care for Complex Pelvic Pain in Women
Chronic pelvic pain is not “just period pain.”
It is often misunderstood, misdiagnosed, and mistreated for years.
At Shree IVF & Endometriosis Clinic, Mumbai, we proudly introduce India’s 1st Dedicated Chronic Pelvic Pain & Neuropelveology Clinic — a specialized centre focused on diagnosing and treating complex pelvic nerve pain, deep endometriosis, and long-standing unexplained pelvic suffering.
This is not symptomatic treatment. This is root-cause precision medicine.
Chronic Pelvic Pain Treatment in India with Dr. Jay Mehta
Treatment at our clinic is a journey, not a quick fix. Because chronic pain involves the complex interaction of organs, nerves, and the brain, a typical chronic pelvic pain treatment protocol in India spans 8 to 12 weeks.
Our goal is to move beyond temporary relief toward a long-term resolution
Our Comprehensive 8–12 Week Protocol
- Rule-Out Protocol: We methodically check every possible pelvic disorder—from deep endometriosis to bladder syndromes—to ensure an accurate diagnosis before treatment begins.
- Multi-Modal Pain Management: We utilize specialized medications and advanced nerve-sparing techniques to "quiet" hyper-responsive pain signals.
- Behavioral & Sleep Therapy: Chronic pain takes a massive emotional and mental toll. We address this through sleep hygiene and specialized coaching to help the brain recover from years of pain.
- Nerve-Sparing Surgery: If surgery is indicated, Dr. Jay Mehta utilizes advanced laparoscopic techniques designed to remove disease while preserving delicate pelvic nerve function, preventing post-operative pain.
The Importance of Early Specialist Consultation
Unfortunately, we frequently see young women who have undergone one or two “diagnostic” laparoscopies elsewhere without any resolution. These patients often come to us having lost years of their lives to ineffective treatments.
This cycle of failed surgeries happens when the focus is only on the organs, ignoring the nerves and the brain's response to pain.
This is precisely why early consultation with a neuropelveology specialist matters. We don't just "take a look"—we provide a definitive plan for recovery.
Stop the cycle of ineffective treatments. Consult India’s leading experts in complex pelvic pain and endometriosis. Call 1800-268-4000 to schedule your consultation.
What Makes Treatment at a Specialized Center Different?
As a referral unit for advanced endometriosis and chronic pelvic pain treatment in Mumbai and across India, we see patterns that general practitioners might miss. Our systematic approach includes:
- Comprehensive evaluation—We combine expert clinical examination with advanced imaging and detailed pain mapping.
- Multidisciplinary care—Your recovery is supported by a team of gynecologists, neurologists, imaging specialists, and pelvic floor therapists.
- Advanced surgical techniques—We specialize in minimally invasive, nerve-sparing procedures that are essential for treating deep-seated pain.
- Long-term follow-up—Chronic conditions often require ongoing management over 7–10 years to ensure quality of life is maintained.
Finding Relief for Chronic Pelvic Pain in Mumbai
As a specialist with over 13 years of experience, I, Dr. Jay Mehta, have seen that the biggest hurdle for women in India is the "diagnostic delay."
On average, it takes 7 to 10 years to reach an accurate diagnosis for chronic pelvic pain (CPP). This happens because the pelvis is a dense "nerve hub," and even microscopic amounts of endometriosis or adenomyosis can cause life-altering agony that standard ultrasounds cannot see.
When you visit us at Shree IVF Clinic, we don't just tell you "everything looks normal." We use advanced diagnostic tools like sonopodography—a specialized water-contrast ultrasound—to find subtle peritoneal lesions that others miss.
Why Patients Travel to Mumbai for Pelvic Pain Treatment
Mumbai has become a central hub for specialized medical care, particularly for women who have exhausted local options. Patients travel to our Mumbai center for access to technology and expertise that isn't widely available:
- India’s 1st Neuropelveology Unit: We offer a specialized field of medicine that focuses on the nerves of the pelvis.
- Advanced Imaging: Beyond standard MRI or ultrasound, we utilize 3D imaging and SonoPODgraphy to identify "invisible" scar tissue and lesions.
- Gold Standard Surgery: Our center is a referral point for laparoscopic nerve decompression and deep-tissue excision, ensuring patients don't need repeat "diagnostic" surgeries.
Whether your pain is caused by peritoneal fibrosis (scar tissue pinching your nerves), pelvic congestion syndrome (vascular pressure), or nerve sensitization due to chronic stress, our approach is always holistic.
We combine precision-based operative laparoscopy to physically free trapped nerves with nerve-calming therapies and sleep management.
Multidisciplinary Pelvic Pain Care
We believe that chronic pain cannot be treated by a single doctor. Our Mumbai-based team provides a holistic, multidisciplinary clinical pathway designed to provide long-term relief where traditional treatments have failed.
| Specialty | Role in Your Recovery |
|---|---|
| Dr. Jay Mehta | Lead specialist in operative laparoscopy and nerve decompression. |
| Dr. Natasha Shah | Neurological management of "pain memory" and central sensitization. |
| Dr. Vismay Pandya | Advanced imaging to map deep endometriosis and peritoneal fibrosis. |
| Rehabilitation | Specialized pelvic floor physiotherapy and behavioral sleep therapy. |
Whether your pain is caused by peritoneal fibrosis (scar tissue pinching your nerves), pelvic congestion syndrome (vascular pressure), or nerve sensitization, our approach combines precision surgery with nerve-calming therapies.
Our goal is a definitive resolution so you can finally return to your normal routine.
Why Choose a Pelvic Pain (Neuropelveology) Clinic?
 Clinic in Mumbai India")
For many women, traditional gynecology reaches a standstill when tests come back "normal" despite persistent, agonizing pain.
This is because standard care often focuses solely on the organs (the uterus and ovaries) while overlooking the complex "electrical wiring" of the pelvis—the nerves.
Conditions such as endometriosis, pelvic nerve disorders, and even large uterine fibroids can contribute to chronic pelvic pain. While many patients initially seek Uterine Fibroid Treatment in India or consultation with an endometriosis specialist, the true source of pain may sometimes lie within the pelvic nervous system rather than the organs alone
What is Neuropelveology?
Neuropelveology is a specialized field of medicine that focuses on the diagnosis and treatment of the pelvic nervous system. It bridges the gap between gynecology, neurology, and neurosurgery.
While a general gynecologist looks at the health of the reproductive system, a neuropelveologist looks at the sensory, motor, and autonomic nerves that control the pelvis.
This approach allows us to identify and treat pain caused by nerve entrapment, irritation, or damage, conditions that standard imaging often fails to detect.
This advanced perspective is particularly important for women who have undergone treatment for conditions such as uterine fibroids or endometriosis but continue to experience pelvic pain.
How a Neuropelveology Clinic Differs from Regular Gynecology
The primary difference lies in the depth of investigation. Traditional diagnostics like MRIs or standard ultrasounds often fail to capture the root cause of pelvic pain when it involves the nervous system.
-
Looking Beyond the Organs: We investigate if your pain is coming from "electrical" issues, such as a nerve being "strangled" by scar tissue or compressed by a previous surgical suture.
-
Nerve Mapping: Instead of just looking for cysts or fibroids, we perform clinical mapping to see if specific nerves (like the Pudendal or Sciatic nerves) are the source of your discomfort.
-
Specialized Expertise: Dr. Jay Mehta is recognized as one of the leading doctors for pelvic pain treatment, endometriosis care, and advanced uterine fibroid treatment in India, combining expertise in gynecological surgery with specialized knowledge of pelvic nerve disorders.
Our Multidisciplinary Treatment Approach
At our center, we believe in conclusive management rather than repeated diagnostic tests. Our dedicated pelvic pain unit follows a multidisciplinary approach, where specialists collaborate to address every layer of pelvic pain.
- Endometriosis Specialists: Experts who perform gold-standard excision surgery to remove endometriosis lesions and reduce inflammatory triggers.
- Neurologists & Neuropelveologists: Specialists who diagnose and treat nerve entrapment, neuropathic pelvic pain, and brain “pain memory.”
- Physiotherapists: Provide targeted pelvic floor rehabilitation to relax and retrain pelvic muscles.
- Pain Management Specialists: Offer multimodal pain relief using specialized medications and therapeutic techniques.
As a leading pelvic pain center in India, we don’t simply perform another diagnostic laparoscopy.
Instead, we provide a specialized clinical pathway designed to identify the true cause of pelvic pain and deliver effective, long-term treatment.
Best Doctors for Chronic Pelvic Pain Treatment & Neuropelveology in Mumbai, India

Dr. Jay Mehta
MBBS, DNB – Obstetrics & Gynecology
Fertility and Endometriosis Excision Specialist, India, Laparoscopic Surgeon (Obs & Gyn)
15+ Years Experience

Dr. Vismay Pandya
MBBS, MS - Obstetrics & Gynaecology
Endometriosis Ultrasound Specialist
11 Years Experience

Dr. Natasha Tipnis Shah
MBBS, MD (Internal Medicine), MRCP(UK), DrNB (Neurology), SCE Neurology UK, PDF Epilepsy (KEMH, Mumbai)( Glasgow, UK)
Neurologist – Pelvic Neuropathic Pain Specialist
15 Years Experience
What Can I Expect from Treatment?
At Shree IVF & Endometriosis Clinic, we believe in setting clear, honest expectations. Because chronic pelvic pain involves the nervous system, recovery is a process of "re-training" the body and brain. It is important to understand that treatment is a partnership between the medical team and the patient.
The Reality of Chronic Management
I want to be honest with you: chronic pelvic pain often requires chronic management. This isn’t a condition where you take a pill for two weeks and forget about it. Because the pain pathways have often been active for years, they require time to stabilize.
Depending on your specific diagnosis and the underlying cause, your personalized journey might include:
- Ongoing Hormonal Therapy: To stabilize the pelvic environment and prevent "flare-ups" caused by your cycle.
- Regular Follow-up Appointments: To monitor nerve recovery and adjust medications as your body heals.
- Specialized Physical Therapy: 12-week sessions to address muscle guarding and pelvic floor tension.
- Stress & Sleep Management: Techniques to lower the "volume" of pain signals in the brain.
- Surgical Intervention: Precision surgery to physically remove disease or free trapped nerves.
Success Stories and Realistic Expectations
While the journey requires commitment, the results can be life-changing. With proper diagnosis and a neuropelveology-focused approach, most of our patients experience significant improvement.
- Surgical Success: Women who have suffered for 7–10 years on ineffective medical management often achieve near-complete pain relief after appropriate surgical intervention, such as nerve decompression or gold-standard excision of endometriosis.
- Quality of Life: Many others find that a combination of hormonal therapy, targeted lifestyle modifications, and stress management dramatically improves their quality of life, allowing them to return to work, exercise, and a normal social life.
What Is Chronic Pelvic Pain, and How Do I Know If I Have It?
Chronic pelvic pain (CPP) is defined as persistent or recurrent pain in the pelvic region lasting for more than six months.
It can be continuous or intermittent, and in many cases, it is linked to underlying conditions such as endometriosis, pelvic inflammatory disease, bladder disorders, or nerve-related issues.
In India, this is an extremely common yet silent epidemic. Unfortunately, it is often ignored or misdiagnosed, leaving women to suffer silently for years.
The Reality of Chronic Pelvic Pain in India
While exact national statistics are rare, our extensive clinical experience suggests that at least 1 in 20 women in India are affected by chronic pelvic pain.
It is a highly disabling disorder that is too often dismissed by families and medical practitioners alike.
This leaves women to navigate a complex journey of emotional, mental, and financial exhaustion alone
At Shree IVF and Endometriosis Clinic, we understand that patients coming to us have often gone through a lot.
Our clinic provides a concerned, supportive environment where your pain is validated and treated with the highest level of clinical expertise. If you are struggling with:
- Persistent pelvic pain that disrupts your routine.
- “Normal” scans that don’t explain your physical discomfort.
- Endometriosis that continues to impact your quality of life despite previous treatments.
It is time for a specialized neurological and neuropelveology approach.
A Specialized Pathway to Relief
Dr. Jay Mehta, a leading pelvic pain specialist in Mumbai, India, offers a comprehensive, nerve-focused clinical pathway designed to provide long-term relief where traditional treatments have failed.
Patient Tip: If you have pelvic pain lasting more than six months, don’t dismiss it as “normal.” You deserve an evaluation from a specialist who understands that pain is often a complex interaction between organs and nerves.
What Are the Common Symptoms of Chronic Pelvic Pain?
Chronic Pelvic Pain (CPP) is more than just a physical sensation; it is a debilitating condition that affects a woman’s quality of life, routine, and emotional well-being.
Typically, it presents as a vague, disturbing, and persistent pain in the pelvic region (area between the belly button (navel) and the hips/pubic bone) that occurs either continuously or intermittently for at least six months.
Because the pelvis contains a complex network of organs and nerves, symptoms of CPP often overlap with those of other conditions, making a specialized assessment by a neuropelveologist essential.
1. Identifying the Nature of the Pain
Patients often describe the symptoms of CPP in non-specific ways, which is why clinical expertise is required to "map" the pain correctly:
- Vague and Nagging: A persistent, heavy ache in the lower abdomen that seems to have no clear trigger
- Debilitating Spikes: Sudden, sharp "shooting" pains that are severe enough to halt daily activities or work.
- Lower Abdominal Overlap: CPP is frequently confused with Irritable Bowel Syndrome (IBS) or general digestive issues because the pain is felt in the same region
2. Common Underlying Triggers in India
In the Indian clinical context, once an expert evaluation is performed, the symptoms of CPP are often found to be linked to the following:
- Endometriosis & Adenomyosis: These are the leading drivers of painful periods (dysmenorrhea), pain during intercourse, and chronic daily discomfort
- Pelvic Congestion Syndrome: This presents as a "dragging" sensation or heaviness in the pelvis, which often worsens after standing for long periods.
- Chronic Inflammation: Long-standing infections (PID) can leave the pelvic environment hypersensitive, leading to constant low-level pain
3. The "Invisible" Symptom: Deep, Tiny Lesions
A critical symptom of CPP that is frequently missed by general gynecologists is the depth of a lesion.
- Small but Severe: Even a tiny endometriotic lesion—if it is deep-seated and invading tissue near a pelvic nerve—can cause agonizing pain.
- The Clinical Gap: Because these lesions are small, they are often dismissed as "minor" or manageable with simple medication. However, their proximity to the nerves means they must be addressed through surgical excision to provide true relief.
4. Ruling Out the "Masks" of Pelvic Pain
To accurately diagnose CPP, we must first ensure the symptoms aren't being "mimicked" by other pelvic organ systems. We meticulously rule out:
- Urologic Causes: Interstitial Cystitis (Bladder Pain Syndrome) or chronic bladder infections.
- Gastrointestinal Causes: Chronic constipation, bloating, or complex intestinal pathologies.
- Musculoskeletal Issues: Pelvic floor muscle spasms or levator ani syndrome.
Our Diagnostic Approach: The 3D Advantage
At the Chronic Pelvic Pain & Neuropelveology Clinic, we don't just ask where it hurts; we use advanced tools to see why it hurts.
- Detailed Clinical Examination: A specialized physical exam to find nerve trigger points.
- Expert 3D Ultrasound: Performed by Dr. Vismay Pandya, this specialized scan is designed to pick up the "tiny but deep" lesions that standard ultrasounds miss.
- Specialized Excision: Led by Dr. Jay Mehta, we focus on removing the pathology entirely, especially when it sits close to the pelvic nerves.
Consult India’s Experts in Pelvic Pain
If you have been living with vague, nagging, or debilitating pelvic pain for over six months, it is time to move beyond general advice and seek a specialized diagnosis. Call Now: 1800-268-4000
Why Do I Experience Severe Pelvic Pain Before and During My Periods?
Pelvic pain associated with the menstrual cycle typically falls under the medical category of dysmenorrhea.
While many women are told that period pain is "normal," a detailed clinical evaluation is essential to distinguish between a simple muscular response and more complex underlying conditions.
Is it the Endometriosis and Adenomyosis Complex?
In many cases, intense pain before and during periods is linked to a complex of Endometriosis (tissue similar to the uterine lining growing outside the uterus) or Adenomyosis (tissue growing into the muscular wall of the uterus).
It is vital that these conditions are strongly ruled out through expert clinical examination and specialized imaging.
A common diagnostic challenge occurs when a lesion is physically small but deeply invasive; if a tiny endometriotic lesion is close to a pelvic nerve, it can trigger debilitating pain. In these situations, the depth of the lesion is more critical than its size, often requiring surgical excision rather than just medical management.
Understanding Spasmodic Dysmenorrhea
In many other situations, a patient may experience a severe amount of pain despite having a uterus that is normal in size, shape, and position.
When clinical assessment confirms there is no evidence of Adenomyosis or Endometriosis, the condition is often identified as Spasmodic Dysmenorrhea.
- The Cause: This occurs due to intense spasms of the uterine muscle that occur specifically during menstruation.
- The Clinical Picture: Even without structural disease or lesions, the intensity of these spasms can be highly disabling and affect a person's routine.
- The Treatment: Once a specialist has carefully and clinically ruled out more complex pathologies, patients suffering from purely spasmodic complaints are usually easily settled down with targeted anti-spasmodic medications.
Why Expert Assessment is Critical?
Because the symptoms of these conditions often overlap, a generic approach to pain management is rarely sufficient.
A specialized evaluation ensures that "invisible" causes of pain—like nerve-invading endometriosis—are not missed, while also ensuring that those with spasmodic pain receive the simple, effective relief they need.
Why Do I Experience Pelvic Pain During Intercourse?
Experiencing pelvic pain during or after sexual activity is medically referred to as Deep Dyspareunia (Painful intercourse). This is a significant clinical marker that requires a specialized diagnostic approach to distinguish between deep-seated physical lesions and complex nerve-related issues.
Is it a Sign of Deep Endometriosis?
One of the most common and critical causes of deep dyspareunia is Deep Infiltrating Endometriosis (DIE).
In these cases, tissue similar to the uterine lining grows deep into the pelvic structures, such as the vaginal wall, the area between the rectum and vagina (rectovaginal septum), or the ligaments supporting the uterus.
Unless endometriosis has been categorically and expertly ruled out through a detailed clinical exam and 3D imaging, it must remain the primary suspicion.
Because these lesions are often "hidden," they require a specialist who understands the depth of the disease rather than just its surface appearance.
Understanding Nerve Entrapment and Surgical History
If endometriosis is not the cause, pelvic pain during intercourse may stem from an alteration in the pelvic nerves. This is frequently linked to a patient's surgical history.
A detailed review of past procedures is essential because:
- Nerve Entrapment: During previous pelvic surgeries, nerves can sometimes become trapped by scar tissue, sutures, or adhesions.
- The Nature of Nerve Pain: Unlike cyclical period pain, pain caused by nerve entrapment is almost always continuous and highly intense.
- NeuroPelveology: Identifying these nerve-related issues requires the expertise of a NeuroPelveologist who can map the sensory and motor nerves of the pelvis to find the exact site of entrapment.
Why Expert Detailing is Necessary?
Passing a comment on the cause of deep dyspareunia without a thorough history is impossible. We must understand exactly what was done in any prior surgeries to determine if the pain is a "virtual extension" of a disease like endometriosis or a result of surgical nerve interference.
At our Pelvic Pain (Neuropelveology) Clinic in Mumbai India, we provide a concerned and emotional assessment to ensure that neither deep lesions nor nerve entrapments are missed, moving you toward a conclusive management plan.
Is it Chronic Pelvic Pain or Deep Endometriosis? Understanding Pain During Bowel Movements
Many patients experience sharp pain or a vague, deep discomfort during bowel movements. While this is often dismissed as a digestive issue, in the context of specialized pelvic care, it is a critical clinical marker that must be investigated thoroughly.
Ruling Out Deep Endometriosis and Rectal Nodules
When a patient reports pain during bowel movements, we must first and strongly consider Deep Infiltrating Endometriosis (DIE). Specifically, we look for involvement of the rectum or the presence of an endometriotic nodule.
- The Nodule Factor: A nodule is a solid mass of endometriotic tissue that can invade the wall of the bowel.
- Specialized Imaging: This cannot be identified through a standard check-up. It must be categorically ruled out using a detailed 3D ultrasound (and sometimes an MRI) performed by an expert who knows how to "map" the bowel for lesions.
The Role of Pelvic Nerve Damage
If a nodule is not present, the discomfort may be neurological. The lateral aspects of the rectum are lined with a complex network of pelvic nerves (part of the inferior hypogastric plexus).
- Nerve Interference: Damage or inflammation of these specific nerves can cause significant pain during the passage of stool.
- Altered Bowel Habits: In many situations, nerve-related issues don't just cause pain; they can give rise to altered bowel movements (constipation or urgency) that mimic Irritable Bowel Syndrome (IBS).
Why a Detailed Pelvic Examination is Mandatory
Labeling a patient with "Chronic Pelvic Pain" without a specific cause is only possible after a rigorous evaluation. A detailed pelvic examination by a specialist is the most important step to:
- Identify the exact site of tenderness.
- Differentiate between a physical lesion (nodule) and a neurological trigger.
- Ensure the patient is not left to seek "unjustifiable" options for a condition that has a clear, treatable medical cause.
Is it Chronic Pelvic Pain or Bladder Pain Syndrome? Understanding Pain During Urination
Pain during urination is a common symptom that is often misdiagnosed as a simple urinary tract infection (UTI). However, when the pain becomes chronic, it is typically classified as Bladder Pain Syndrome (BPS).
Identifying the root cause requires a specialized evaluation of the bladder wall and the nerves that control it.
Understanding Bladder Pain Syndrome (BPS)
Bladder pain syndrome is an umbrella term for chronic discomfort, pressure, or pain related to the bladder. It is extremely common in patients with underlying bladder pathologies, including:
- Interstitial Cystitis (IC): The condition is often caused by age-related changes in the protective lining of the bladder. When this lining breaks down, toxins in the urine can irritate the bladder wall, leading to chronic inflammation and severe pain.
- Diabetic-Induced Cystitis: Patients with diabetes are at a higher risk for various types of cystitis. High blood sugar can lead to nerve changes or recurrent infections that eventually manifest as chronic bladder pain.
The Nerve Connection: Why Urination Becomes Painful
In many cases of chronic pelvic pain, the bladder itself may be healthy, but the pelvic nerves that supply the bladder are inflamed or damaged. This can result in:
- Urgency and Frequency: Feeling the need to urinate even when the bladder is nearly empty.
- Referred Pain: Pain that feels like it is in the bladder but actually originates from the pelvic wall or nearby endometriotic lesions.
Why a Conclusive Diagnosis Matters
Labeling a patient with "Chronic Pelvic Pain" without investigating the bladder is incomplete. At our Pelvic Pain (Neuropelveology) Clinic, we perform a detailed assessment to rule out BPS (Bladder Pain Syndrome) and IC (Interstitial Cystitis) before finalizing a treatment plan.
Our approach focuses on conclusive management because patients with these symptoms often experience significant emotional and financial stress. This includes:
1. Specialized Urinalysis and Imaging: To check for age-related or diabetic-induced changes in the bladder.
2. Neurological Mapping: To ensure the pain isn't stemming from the autonomic nerves of the pelvis.
3. Multimodal Therapy: Using a mix of medical treatment and behavioral and sleep therapy to help with the severe pain from chronic bladder discomfort, which may involve changing medications, cognitive behavioral therapy, and good sleep habits to enhance patient results.
Stop managing the symptoms and start treating the cause. Reach out to India’s premier Pelvic Pain (Neuropelveology) Clinic today for a definitive path forward. Contact for Appointments: 1800-268-4000
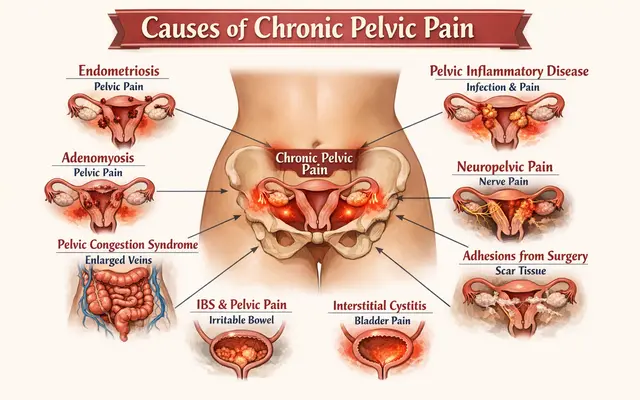
What Are the Causes of Chronic Pelvic Pain?
Chronic pelvic pain can arise from several conditions affecting the pelvic organs, nerves, muscles, or digestive system.
Common causes include gynecologic conditions like endometriosis and adenomyosis, gastrointestinal disorders such as irritable bowel syndrome, musculoskeletal problems involving the pelvic floor muscles, and nerve-related pain like pelvic nerve entrapment.
Proper diagnosis is essential to identify the underlying cause and guide effective treatment.
What Are the Gynecologic Causes of Chronic Pelvic Pain?
In the Indian clinical context, Chronic Pelvic Pain (CPP) is frequently a "mask" for undiagnosed gynecologic conditions. Because many of these diseases have a long diagnostic lead time—often 5 to 6 years—many women suffer needlessly, thinking their pain is simply a part of life.
Identifying the root cause requires a specialist who can distinguish between general discomfort and specific pathological triggers.
1. Endometriosis: The Hidden Epidemic
Endometriosis is the most common differentiator for patients with chronic pelvic pain. In India, it is frequently missed in early stages, leading to patients moving from doctor to doctor without a proper diagnosis.
The Reality: When endometriosis is left unaddressed, it progresses into a chronic pain state that affects the entire pelvic nervous system.
2. Adenomyosis: The Missed Diagnosis
Often co-occurring with endometriosis, adenomyosis (in which the uterine lining grows into the muscular wall of the uterus) is the second most commonly missed disease.
It causes heavy, painful periods and a constant, dull pelvic ache that persists throughout the month until correctly diagnosed via specialized 3D ultrasound.
3. Pelvic Inflammatory Disease (PID)
In India, PID is extremely common across all socioeconomic strata.
- The Environmental Factor: The prevalent weather conditions, specifically high humidity, contribute to the frequency of both acute and chronic pelvic infections. If not treated conclusively, these infections lead to permanent scarring and chronic inflammation.
4. Ovarian Cysts and Pain
While large cysts are easy to spot, most benign ovarian cysts are actually painless unless they rupture (hemorrhage) or twist (torsion).
- The Clinical Marker: If an ovarian cyst is associated with persistent chronic pelvic pain, it is most commonly an endometrioma (a "chocolate cyst" related to endometriosis).
5. Pelvic Adhesions and Post-Surgical Nerve Entrapment
Adhesions (internal scar tissue) are very common causes of CPP, especially in patients with a history of the following:
- Previous Cesarean sections.
- Open surgeries for other medical conditions.
The Specialist’s Warning: Often, patients are operated on by practitioners who do not specialize in advanced pelvic surgery. This can result in post-surgical nerve entrapment, where a nerve is accidentally caught in a suture or scar tissue.
This creates a severe, continuous type of chronic pelvic pain that only a specialized pain clinic can address through a detailed review of surgical history and a neurological pelvic exam.
If you have had surgery but your pain has worsened or remained the same, it is vital to have your case reviewed by a neuroPelviology expert, a specialist who focuses on the neurological aspects of pelvic pain.
At our clinic, we don't just look at the organs; we look at the previous surgical footprints to identify if nerve entrapment is the true cause of your suffering.
Consult with Dr. Jay Mehta, India’s leading expert in complex pelvic pain and nerve-sparing surgery.
Gastrointestinal Causes of Chronic Pelvic Pain
It is common for pelvic pain to be mistaken for digestive issues, leading many patients to spend years seeking treatment for gastrointestinal (GI) disorders while the actual cause remains rooted in the pelvic structures or nerves.
1. Irritable Bowel Syndrome (IBS) and Pelvic Pain
Irritable Bowel Syndrome is a condition frequently characterized by vague abdominal symptoms, including bloating, cramping, and altered bowel habits.
It is often considered a psychosomatic disorder that significantly affects high-stress "Type A" personalities. However, because IBS lacks an obvious physical cause in the bowel, it is frequently confused with more severe inflammatory conditions such as:
- Ulcerative Colitis
- Crohn’s Disease
2. The "IBS" Trap: Missing Bowel Endometriosis
The most critical diagnostic challenge in India is distinguishing between true IBS and bowel endometriosis. Because the symptoms are nearly identical, many women are treated for years for "stomach issues" when they actually have endometriotic nodules invading the bowel wall.
- The Diagnostic Gap: Identifying bowel nodules requires extreme technical expertise in specialized 3D pelvic ultrasound. Standard scans often miss these nodules, leading to a "normal" report despite the patient’s severe suffering.
- National Referrals: At our clinic, we frequently see patients referred from across the country who were previously misdiagnosed with IBS. In these cases, surgical management (excision) of the bowel nodules is the only way to achieve a truly pain-free life.
3. Chronic Pelvic Pain and Bowel Dysfunction
When the pelvic nerves—specifically those along the lateral aspect of the rectum—are damaged or inflamed, it can mimic GI distress. This creates a cycle of "altered bowel movements" that medications for IBS cannot fix.
Musculoskeletal Causes of Chronic Pelvic Pain
Not all pelvic pain originates from the internal organs; frequently, the source is the structural "cradle" of the pelvis—the muscles, fascia, and nerves that support the body. Identifying these triggers requires a specialist who understands the mechanical and neurological interplay of the pelvic floor.
1. Pelvic Floor Dysfunction and Myofascial Pain
Pelvic floor dysfunction is a broad term encompassing a range of symptoms caused by the inability to correctly relax and coordinate the pelvic floor muscles. When these muscles or the endopelvic fascia (the connective tissue supporting the organs) become weak or overly tense, it creates a chain reaction of pain.
- Nerve Stretch and Tension: Dysfunction in the pelvic floor induces a mechanical stretch on the critical pelvic nerves. Specifically, this affects the hypogastric nerves and the nerves originating from the Lumbo-Sacral plexus.
- The Sensation: This tension often manifests as a deep, aching chronic pelvic pain that may worsen with movement, posture changes, or long periods of sitting.
2. The Role of Atypical Prolapse
While many associate "prolapse" with obvious physical displacement, certain atypical natures of prolapse can occur internally. These subtle shifts in organ positioning can put undue pressure on the pelvic nervous system, giving rise to significant chronic pain that standard screenings often overlook.
3. A Multi-Modal Treatment Approach
At our Pelvic Pain (Neuropelveology) Clinic, we do not rely solely on one method of relief. Our treatment for musculoskeletal pain is highly individualized:
- Detailed Clinical Examination: This is the most critical step. A specialized physical exam allows us to identify trigger points in the myofascial tissue and detect atypical prolapse.
- Nerve Relaxation & Rehabilitation: We utilize targeted nerve relaxation medications combined with specialized pelvic floor exercises to reduce muscle guarding and nerve tension.
- Surgical Management: In cases where atypical prolapse or structural weakness is the primary driver, surgical intervention may be warranted to restore the pelvic architecture and provide a permanent path to a better quality of life.
Neuropathic Causes of Chronic Pelvic Pain
When pelvic pain becomes sharp, burning, or electric-like, the cause is often neuropathic—meaning the nerves themselves are injured, inflamed, or compressed. Identifying these specific nerve pathways is the hallmark of the NeuroPelveology approach.
1. Pudendal Neuralgia
Pudendal neuralgia is widely considered one of the most painful conditions a person can experience. It occurs when the pudendal nerve—the main nerve of the perineum—becomes compressed or irritated as it travels through the pelvis.
- The Alcock Canal Connection: The most frequent site of compression is at the anatomical exit of the pelvis, known as the Alcock Canal.
- The Role of Endometriosis: While many factors can cause this compression, Endometriosis is a leading culprit. Endometriotic lesions can grow around the nerve or create scar tissue that "strangles" it at this critical exit point.
- Symptoms: Patients often describe a stabbing or burning pain that is significantly worse when sitting and may improve when standing or lying down.
2. Diagnosis and Surgical Precision
Treating pudendal neuralgia effectively requires a "detective-like" approach to diagnosis. Because the nerve is deep within the pelvic structure, standard gynecology often misses the signs.
- Careful Planning: Diagnosis involves mapping the pain to the exact distribution of the pudendal nerve. At our clinic, this is supported by detailed clinical examinations and high-resolution imaging.
- Definitive Surgical Management: Once the site of compression is identified, surgical decompression is often the most effective treatment.
By surgically correcting the pathology—such as removing an endometriotic nodule or releasing the nerve from the Alcock Canal—we can provide near-instant relief from this debilitating pain.
Pelvic Nerve Entrapment: When "Hidden" Nerves Cause Chronic Pain
Nerve entrapment is a severe and often misdiagnosed cause of chronic pelvic pain. It occurs when a pelvic nerve is physically compressed or "strangled," preventing it from functioning correctly and sending constant pain signals to the brain.
1. How Does Nerve Entrapment Occur?
There are two primary ways a pelvic nerve becomes trapped:
- Disease-Driven Entrapment: Typically caused by Endometriosis. Endometriotic lesions can grow directly onto a nerve or create inflammatory scarring that pulls and compresses the nerve fibers.
- Post-Surgical Adhesions: This is a frequent complication of previous pelvic surgeries (like C-sections or hysterectomies). Internal scar tissue (adhesions) can form around a nerve, or in some cases, a nerve can be inadvertently caught in a surgical suture.
2. Common Sites of Entrapment
The pain location often depends on which specific nerve is being compressed:
- Sciatic Nerve: Entrapment usually occurs at its exit point in the pelvis. This can cause pain that radiates from the pelvis down into the leg.
- Pudendal Nerve: Often trapped as it exits the pelvis (near the Alcock Canal), leading to severe pain in the perineum that worsens when sitting.
- Femoral Nerve: Compression here can lead to pain or weakness in the front of the thigh and groin area.
3. The Path to Relief: From Medication to Release
Because nerve entrapment causes such a high intensity of pain, we follow a progressive treatment protocol:
- Initial Management: To provide immediate relief, we often start with a combination of high-strength painkillers and nerve relaxants. These help "quiet" the overactive pain signals.
- The Surgical Solution: While medication can manage symptoms, it does not fix the physical compression. Most patients with confirmed entrapment require Surgical Decompression.
- Expert Release: Using advanced NeuroPelveology techniques, the surgeon identifies the exact site of compression and carefully releases the nerve from the surrounding adhesions or endometriotic tissue. This "release" is often the only way to achieve a permanent, pain-free life.
Central Sensitization: When the Brain Remembers the Pain
One of the most frustrating experiences for a patient is having a "clean" pelvic scan or a "successful" surgery, yet continuing to feel chronic pelvic pain. In these cases, the cause is often Central Sensitization.
This condition explains why the body continues to signal pain even after the physical injury or disease (like endometriosis) has been completely treated.
1. What is Central Sensitization?
Central Sensitization is a process where the central nervous system (the brain and spinal cord) becomes "hypersensitive." Over time, if the body is exposed to chronic pain, the brain particularly adapts to a certain threshold of stimulus.
- Hyper-Response: The brain begins to "hyper-respond" to normal signals. What should be a mild sensation is interpreted by the brain’s complex pathways as severe pain.
- Pain Memory: Even after an endometriosis specialist has surgically removed every lesion, the brain’s "alarm system" remains stuck in the "on" position.
2. Why We Must First "Clear" the Pelvis
As chronic pelvic pain specialists, our first priority is always to ensure the pelvis is normal. We must completely take out the obvious physical causes—such as endometriotic nodules or nerve entrapments—before we can effectively address the brain's response.
If a physical trigger still exists in the pelvis, it will continue to "feed" the central sensitization. Once the pathology is cleared, we can focus on "re-training" the nervous system.
3. A Multidisciplinary Approach to Re-Training the Brain
Because the arrangement of central sensitization in the brain is extremely complex, it cannot be treated with surgery alone. We utilize a multidisciplinary team approach to help the brain unlearn these pain patterns:
- Neurologists & Pain Management Specialists: To provide medical support that helps stabilize hyper-responsive nerve pathways.
- Cognitive Behavioral Therapy (CBT): Guiding the patient through techniques that help change the emotional and cognitive response to pain signals.
- Education & Distraction: We educate the patient on how to respond to particular sensations and use distraction techniques to "quiet" the brain's alarm system.
- Sleep & Behavioral Therapy: Essential components of our 8–12 week system to reset the body's threshold for pain.
How is Chronic Pelvic Pain Diagnosed?
The diagnosis of Chronic Pelvic Pain (CPP) is a meticulous process that balances listening to a patient’s lived experience with high-precision imaging.
Because CPP often presents with non-specific or "random" symptoms, a standard physical check-up is rarely enough to find the root cause.
1. The Power of a Detailed Patient History
The essence of a CPP diagnosis begins with a "good history." We pay close attention to the way a patient describes her pain, as these non-specific complaints often point directly to the source:
- The "Nagging" Ache: Pain that seems to occur randomly during the day or while at work.
- Activity-Triggered Pain: Discomfort that spikes during specific tasks, such as driving home or sitting for long periods.
- Vague Tracking Pain: Discomfort that "tracks" or moves, appearing at different times and disturbing the patient's routine.
2. Specialized Ultrasound: The Diagnostic Pillar
In our clinic, the primary diagnostic tool is an excellent ultrasound. While many patients are told their scans are "normal" elsewhere, the difference lies in the expertise of the specialist performing the scan.
- The Expert Advantage: A well-done ultrasound by a specialist is excellent for picking up tiny endometriotic lesions and other subtle issues that may be responsible for the pain.
- A Unique Approach: At our center, Dr. Vismay Pandya performs these high-resolution ultrasounds. His specialized skills offer a unique approach to diagnosing and managing the disease, ensuring that even the smallest pathologies are identified.
- Why Not MRI? We typically do not recommend an MRI for these cases, as a specialized ultrasound is often more effective at identifying the fine details of pelvic lesions.
3. Specialized Testing for Nerve and Bowel Involvement
If the initial history and ultrasound suggest that the pain involves more than just the reproductive organs, we utilize targeted assessments:
- Dermatome-Based Assessment: If we suspect nerve involvement, we perform a specialized physical exam to map pain along specific nerve pathways (dermatomes). This is crucial for identifying nerve entrapment or inflammation.
- Gastrointestinal Review: In cases where symptoms overlap with bowel movements, we may involve a Gastroenterologist to rule out colon-based issues and ensure a comprehensive diagnosis.
Why a Conclusive Diagnosis Matters
Labeling a patient with "Chronic Pelvic Pain" is only the beginning. Our goal at the Pelvic Pain (Neuropelveology) Clinic is to move from a symptom to a cause.
By combining the expert sonography of Dr. Vismay Pandya with a deep dive into your surgical and clinical history, we provide a roadmap for recovery.
What Tests Are Done for Chronic Pelvic Pain?
Diagnosing Chronic Pelvic Pain (CPP) requires more than just a standard check-up. At our specialized clinic, we follow a rigorous testing protocol designed to find "invisible" pathologies that general screenings often miss.
1. Specialized Pelvic Ultrasound: The First Step
The most important diagnostic tool we use is a high-resolution ultrasound. While many patients come to us with "normal" scans from other centers, the accuracy of an ultrasound depends entirely on the skill of the person performing it.
- Expert Precision: In our team, Dr. Vismay Pandya performs these ultrasounds. His specialized skills allow us to pick up tiny endometriotic lesions and other subtle structural issues that are the true culprits behind pelvic pain.
- Why We Avoid MRI: For most CPP cases, we typically do not recommend an MRI. A well-executed ultrasound by a specialist is often far superior in identifying the fine details of pelvic disease and directing the management plan.
2. Neuropathic Testing: Dermatome-Based Assessment
When we suspect that the pain involves the pelvic nerves (such as in cases of nerve entrapment or pudendal neuralgia), we perform a dermatome-based assessment.
- Pain Mapping: This is a specialized physical examination where we map the patient’s pain along specific nerve pathways (dermatomes). By identifying exactly where the sensation is altered or heightened, we can pinpoint which pelvic nerve is affected.
- Clinical Significance: This test is essential for patients whose pain is continuous or follows a specific surgical history.
3. Multidisciplinary Rule-Outs
Because the pelvis contains multiple organ systems, we sometimes need to look beyond gynecology to ensure a conclusive diagnosis:
- Gastrointestinal Review: In cases where symptoms overlap with bowel movements or abdominal discomfort, we involve a Gastroenterologist.
This allows us to rule out colon-based symptoms and ensure the issue isn't purely digestive before we proceed with pelvic treatment.
- Urologic Evaluation: If the pain is centered around urination, we may also assess the bladder for conditions like Interstitial Cystitis.
If you have undergone routine tests but your pain remains unexplained, it is time for a specialized diagnostic review.
Our clinic, led by Dr. Jay Mehta, is dedicated to providing the expert detailing required to move from chronic suffering to a clear recovery plan. 📞 Schedule Your Diagnostic Review: 1800-268-4000
Book a consultation with Dr. Jay Mehta, a leading pelvic pain and endometriosis specialist in Mumbai, India
When is laparoscopy needed?
The medical approach to chronic pelvic pain has evolved significantly. In the past, "diagnostic laparoscopy" was often performed just to "take a look" inside the pelvis. Today, the focus has shifted toward a more purposeful and active surgical strategy.
1. From Diagnostic to Operative Surgery
The modern approach moves away from unnecessary diagnostic procedures. Instead, we prioritize operative laparoscopy. This means that when we go in for surgery, the goal is to identify and treat the pathology in the same session.
- No More "Wait and Watch": Rather than simply waiting for symptoms to worsen or performing a surgery with no plan for treatment, we use laparoscopy as a definitive tool for resolution.
- Addressing "Small" Lesions: A common misconception is that only large cysts or masses require surgery. However, in the case of endometriosis, even a tiny, "invisible" lesion can cause debilitating pain if it is located near a pelvic nerve. These small but highly symptomatic lesions require expert surgical management to be completely excised.
2. When Surgery Becomes Necessary
Laparoscopy is typically recommended when noninvasive treatments (like medication or pelvic physiotherapy) haven't provided relief or when imaging suggests a physical cause that requires manual correction. Key indications include the following:
- Suspected Deep Endometriosis: When specialized 3D ultrasound identifies nodules that cannot be treated with hormones alone.
- Nerve Entrapment: When a patient’s history and pain mapping suggest a nerve is being compressed by scar tissue or disease.
- Persistent Pelvic Pain: When the pain is disabling and a "clean" ultrasound doesn't match the severity of the patient's symptoms.
3. The Goal: A Pain-Free Life
At our Pelvic Pain (Neuropelveology) Clinic, led by Dr. Jay Mehta, minimally invasive surgery is performed with the "gold standard" technique of excision. By completely removing the diseased tissue rather than just burning the surface (ablation), we ensure the best possible long-term outcome for the patient.
Medical Treatment for Chronic Pelvic Pain: Medications and Hormones
While surgery is often necessary for physical lesions, medical management plays a vital role in stabilizing the pelvic environment and reducing the "volume" of pain signals sent to the brain. At our specialized clinic, we move beyond simple painkillers to a targeted pharmacological approach.
1. Pain Relief and Nerve Relaxation
Managing Chronic Pelvic Pain (CPP) requires addressing both the physical muscle response and the underlying nervous system.
- Anti-Spasmodic Medications: These are extremely helpful for women experiencing "spasmodic" pain, where the uterus or pelvic muscles are in a state of constant contraction.
- Nerve Relaxants: For patients with neuropathic pain (nerve-related), we frequently use medications that quiet hyper-responsive nerves. This is essential for breaking the cycle of constant pain signaling.
2. Hormonal Stabilization Strategies
Hormones often act as a "fuel" for pelvic pain, especially in cases of endometriosis or adenomyosis. We use hormonal therapy to stabilize the pelvic axis and reduce sensitization.
- Oral Contraceptives: Often the first line of treatment for younger women to regulate the cycle and reduce inflammatory triggers.
- Retrogesterone (Duphaston): Our clinical approach has shifted toward the use of Duphaston. This medication helps stabilize the hormonal environment and reduces "pelvic sensitization"—the process where the pelvis becomes hypersensitive to hormonal shifts, leading to sudden, shooting pains.
- GnRH Analogues: In severe or refractory cases, we may rarely use GnRH analogues. These medications temporarily "switch off" the menstrual cycle entirely. By inducing a period-free state, we can significantly reduce hormone-induced sensitization and give the pelvic nerves time to heal.
3. Reducing Pelvic Sensitization
The goal of medical treatment is not just to mask the pain, but to perform "Nerve Desensitization." By combining nerve relaxants with hormonal stabilizers like retrogesterone, we aim to lower the body’s pain threshold, making daily activities more manageable while we work toward a conclusive diagnosis or surgical plan.
Non-Drug Therapy for Chronic Pelvic Pain
While medications and surgery address the physical and hormonal triggers of pain, non-drug therapies are essential for "re-training" the body and brain. At our clinic, these are not just optional extras—they are integrated components of our 8–12 week recovery system.
1. Pelvic Floor Physiotherapy
Pelvic floor physiotherapy involves specialized exercises and manual techniques to address muscle tension and weakness in the pelvic cradle.
- The Synergistic Effect: While the effects of using physiotherapy alone may not be significant, it is exceptionally effective when used as a complementary service alongside medical or surgical treatment.
- Commitment to Recovery: Physical rehabilitation is a marathon, not a sprint. A typical course requires at least 12 weeks of consistent sessions to see a meaningful reduction in pain and improved muscle coordination.
2. Cognitive Behavioral Therapy (CBT)
CBT is a mainstay treatment, particularly for patients where no obvious physical cause requires surgery, or for those dealing with Central Sensitization.
- Rewiring the Brain: CBT is excellent for breaking established pain pathways. It works by "resetting" the brain’s signaling pathways back to normal, changing how the mind perceives and responds to pain stimuli.
- A Team Effort: This involves our psychologists and neurologists working together to help the patient explicitly understand how to alter their internal pain mapping.
- Tools for Success: Patients are taught distraction techniques and are encouraged to maintain pain diaries. Success depends heavily on the patient’s initial pain cognition, age, and motivation, as this process requires significant patience.
3. Lifestyle Management & Holistic Care
Education and stress release are vital for every patient suffering from chronic pelvic pain. We provide constant coaching to help patients reduce their overall pain sensitivity.
- Holistic Benefits: We integrate breathing exercises and yoga into our protocols. These practices help calm the nervous system and improve pelvic blood flow.
- Coaching Sessions: Specialized coaching sessions typically last between 10 to 13 weeks. These sessions focus on reducing the emotional response to pain and empowering the patient with self-management tools.
- Stress Reduction: Lowering cortisol and adrenaline levels through lifestyle changes is essential for preventing the "flare-ups" often associated with chronic pelvic conditions.
How Can Sleep Therapy Help Manage Chronic Pelvic Pain?
At our specialized clinic, we recognize that physical treatment is only one half of the recovery journey. A large proportion of our management strategy is focused on Sleep Therapy. For a patient with chronic pelvic pain, achieving high-quality, deep sleep is not a luxury—it is a mandatory part of the neurological recovery process.
1. Why Sleep is Essential for Brain Recovery
Chronic pain places the brain in a constant state of "high alert" or hyper-vigilance. Over time, this exhausts the nervous system and lowers your pain threshold, making even mild sensations feel intense.
- Neurological Reset: Deep sleep provides the brain with the necessary environment to recover from persistent pain sensations. It allows the central nervous system to "reset" and reduces the chemical triggers of inflammation.
- Breaking the Pain-Insomnia Cycle: Pain often prevents sleep, and a lack of sleep makes the brain more sensitive to pain the following day. Sleep therapy aims to break this debilitating cycle.
2. Our Approach to Sleep Management
To ensure an excellent recovery, we incorporate targeted sleep support into our 8–12 week multidisciplinary protocol:
- Melatonin Supplements: We frequently use melatonin supplements as a safe and effective way to help patients transition into a deep sleep state. Melatonin is a natural hormone that regulates the sleep-wake cycle and has been shown to have protective effects on the nervous system.
- Sleep Hygiene Education: Guiding the patient on how to create an environment conducive to rest, reducing "blue light" exposure, and establishing a routine that signals the brain it is time to heal.
- Behavioral Therapy: Addressing the anxiety and stress that often accompany chronic pelvic pain, ensuring the mind is as rested as the body.
3. A Multi-Modal Path to Healing
Sleep therapy is a core component of the Chronic Pelvic Pain System led by Dr. Jay Mehta. By ensuring your brain has the rest it needs, we enhance the effectiveness of our other treatments—whether they are medical, physical, or surgical.
Surgical Treatment for Chronic Pelvic Pain
Surgery for chronic pelvic pain is recommended when medications, physiotherapy, and non-surgical treatments fail to relieve symptoms.
Minimally invasive laparoscopic surgery helps identify and treat the root cause of pain, such as endometriosis, adenomyosis, pelvic nerve entrapment, or adhesions, by removing diseased tissue and decompressing affected pelvic nerves.
When conservative treatments like medication and physiotherapy are insufficient, surgical intervention becomes the definitive path to relief.
At our specialized clinic, surgery is not just about “looking inside”—it focuses on precision anatomical correction and pelvic nerve decompression to treat the underlying cause of pain.
1. Operative Laparoscopy: The Treatment of Choice
- Laparoscopic surgery: It is recommended when there is a confirmed or strongly suspected physical cause for pelvic pain, such as nerve impingement, pelvic adhesions, deep infiltrating endometriosis, or structural abnormalities.
- Targeted Decompression: If a pelvic nerve is compressed by scar tissue or trapped by a previous surgical suture, operative laparoscopy allows surgeons to carefully release the pressure and restore normal nerve function.
- The Healing Timeline: Many patients experience noticeable improvements soon after surgery.
However, when nerves have been compressed for a long time, they may develop neuropraxia, a temporary nerve injury.
In such cases, full recovery may take 3–4 months as the nerve gradually heals.
2. Specialized Endometriosis & Adenomyosis Surgery
As a premier referral unit for Endometriosis and Adenomyosis in India, we believe that excision surgery remains the "Gold Standard" treatment for pain relief when indicated.
- Complete Excision: Unlike standard "burning" (ablation) of lesions, we focus on the complete removal of diseased tissue. This is especially critical for deep infiltrating endometriosis that involves the bowel, bladder, or pelvic nerves.
- Specialized Management: Our unique surgical approach ensures that the disease is managed effectively at its root, significantly reducing the chance of recurrence and chronic symptoms.
3. Adhesiolysis and the Role of the Omentum
Adhesions (internal scar tissue) from past surgeries—like C-sections or open abdominal procedures—are a major cause of chronic pain. While Adhesiolysis (cutting the adhesions) is a common procedure, we must address the reality of recurrence.
- Adhesion Reformation: There is currently no medication or therapy that can completely prevent adhesions from reforming after they are cut. This is a significant challenge for patients who have undergone multiple prior surgeries.
- The Omentectomy Option: In many complex cases, performing an Omentectomy (removing a portion of the fatty tissue layer in the abdomen) is a superior option.
- Why it Works: The "pull" or tension on the omentum when it is stuck to pelvic organs contributes significantly to the patient's pain. By removing the source of this tension, we can offer more sustainable relief than simple adhesiolysis alone.
When Is Surgery Necessary for Chronic Pelvic Pain?
Surgery for chronic pelvic pain is considered when persistent pain continues despite normal scans, medications, or physiotherapy.
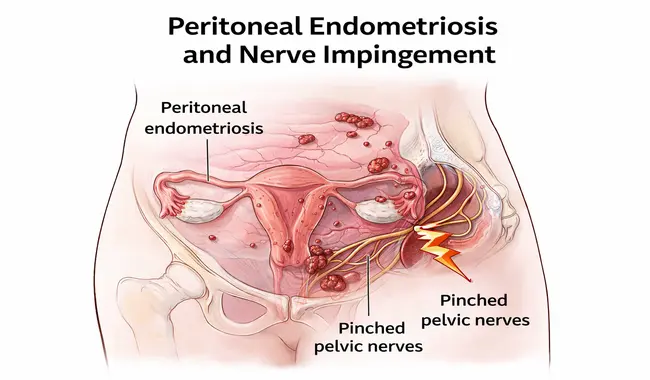
In many cases, minimally invasive laparoscopy helps identify hidden conditions such as peritoneal endometriosis or pelvic nerve impingement.
Removing the affected tissue can relieve nerve pressure and significantly improve pain.
One of the main reasons surgery is performed even when imaging tests appear normal is to identify microscopic or peritoneal endometriosis.
Although these lesions may appear extremely small on the surface, they can still place significant pressure on nearby pelvic nerves, leading to severe and persistent pain.
- The Surgical Technique: Rather than simply inspecting the pelvis, surgeons perform a wide local excision of the affected peritoneal tissue to remove the disease completely.
- The Result: By removing the affected tissue with adequate margins, the pressure on surrounding pelvic nerves is relieved, often leading to substantial and sometimes immediate pain relief.
This approach is particularly important in cases of peritoneal endometriosis associated with pelvic nerve irritation or nerve impingement.
When Should Surgery Be Avoided?
Surgery is not always necessary for chronic pelvic pain. Many patients respond well to non-surgical treatments when the underlying cause is identified.
For example:
- Pelvic congestion syndrome may improve with hormonal therapy.
- Pelvic infections often respond to appropriate antibiotic treatment.
- Stress-related or functional pelvic pain may improve with lifestyle changes, physiotherapy, or holistic therapies.
Because chronic pelvic pain can have multiple causes, careful evaluation is essential before recommending surgery.
Why Specialist Evaluation Matters
If you have been experiencing long-standing pelvic pain, consulting a specialist who understands the complex causes of chronic pelvic pain is crucial.
Chronic pelvic pain specialists, such as Dr. Jay Mehta, focus on identifying the precise cause of pain through detailed clinical evaluation and advanced diagnostic techniques
A specialized approach allows for accurate diagnosis and targeted treatment, whether that involves medical therapy, lifestyle management, or minimally invasive surgery.
Our experience shows that holistic management—combining precise surgical techniques with long-term follow-up and supportive care—provides the best outcomes for patients suffering from chronic pelvic pain.
Do All Patients with Chronic Pelvic Pain Require a Diagnostic Laparoscopy?
In modern gynecology, the role of a "diagnostic" laparoscopy has evolved significantly.
At Shree IVF & Endometriosis Clinic, we believe that surgery should move straight from diagnosis to treatment in a single step.
We only consider laparoscopy after we have ruled out every other possible cause of pain. When we do go in, the goal is usually operative laparoscopy—to find and remove the source of the pain immediately.
Can Endometriosis Infiltrate Nerves and Cause Chronic Pelvic Pain?
Yes, endometriosis has a notorious ability to affect the millions of nerves that exit through the pelvis. In fact, the concentration of nerves in the pelvic region is so high that we often joke that the pelvis is simply a collection of nerves with a few organs placed in between them.
When endometriosis is present, it triggers fibrosis (thick scarring), which can irritate or physically encase these delicate nerve pathways.
How does Endometriosis Affects Your Pelvic Nerves?
It is not always a direct infiltration; often, the pain is caused by the "neighborhood" effect:
- Ligament Involvement: We frequently see endometriosis involving the uterosacral ligaments. This causes "puckering" and scarring that pulls on the inferior hypogastric nerves, which supply the uterus, vagina, bladder, and rectum.
- Nerve Irritation: Even a small amount of fibrosis is enough to irritate these nerves, leading to deep pelvic pain and referred pain that can be felt in other parts of the body.
Infiltration of Major Nerve Roots (Sciatic & Obturator)
In more advanced cases, lateral pelvic wall endometriosis can go further:
- Sciatic Nerve & Nerve Roots: Endometriosis can encase or infiltrate the roots of the sciatic nerve.
- Obturator Nerve: This often leads to severe pain associated with the muscles of the lower limb, which typically aggravates significantly during menstruation.
Because these symptoms are so severe, they are often easier to identify. At Shree IVF & Endometriosis Clinic, as a referral unit for advanced cases in India, we perform systematic neurological evaluations of the lower limbs to map out exactly how the nerves are being affected.
The Specialist Approach to Treatment
Once we accurately diagnose nerve involvement, the treatment involves minimally invasive surgery (laparoscopy). The goal is twofold:
- Decompression: Relieving the physical pressure on the nerve.
- Neurolysis: Carefully removing the fibrosis from the nerve itself.
This precision-based approach offers almost immediate pain relief. While it is normal to experience some tingling or numbness for 6 to 8 weeks following the procedure as the nerves heal, most patients achieve a complete recovery through a combination of surgery and specialized physiotherapy.
Why Does Pelvic Pain Occur Even When the Pelvis Appears Healthy?
It can be incredibly frustrating to experience severe pain only to be told that your scans or laparoscopy show a "clean pelvis."
At Shree IVF & Endometriosis Clinic, we understand that a lack of visible disease does not mean the pain isn't real.
Because the pelvis is a massive hub for the nervous system, pain can often be referred or caused by issues that don't show up as typical "masses" or "lesions."
1. Nerve Hyper-Activation and Referred Pain
The nerves in your pelvis are interconnected with the rest of your body. If you have a severe injury or chronic pain in your spinal cord, upper abdomen, or lower limbs, the nerve roots inside the pelvis can become hyperactivated.
This creates a "short circuit" where your brain perceives pain in the pelvis, even though the original injury is elsewhere. Before suggesting surgery, we thoroughly investigate these pathways to ensure we aren't treating the wrong area.
2. Pelvic Congestion Syndrome (Vascular Pain)
Sometimes the issue isn't the organs but the blood flow. Pelvic congestion occurs when the veins in the pelvis become enlarged (hypervascularity). These swollen veins put constant pressure on the tiny, sensitive nerves nearby.
- How we find it: A standard ultrasound might miss this, but an ultrasound with Doppler allows us to see the blood flow and identify congestion.
- Treatment: Many patients find relief through specific pelvic exercises or hormonal therapy (like progesterone) to reduce vascular swelling.
3. Chronic Pelvic Infections
Hidden or low-grade infections can cause significant inflammation. While there may be no visible "growth," the inflammation causes hypervascularity that irritates pelvic nerves.
A clinical examination and specific testing allow us to identify and treat these with targeted antibiotics, often resolving the pain without the need for surgery.
When Is a Diagnostic Laparoscopy Still Necessary?
If hormonal therapy, antibiotics, and exercises provide no relief, we may still consider a diagnostic laparoscopy.
Our goal here is to look for "Subtle Peritoneal Endometriosis"—tiny implants that are invisible to even the best imaging but are enough to cause central pain sensitization.
How Does Stress Affect the Manifestation of Pelvic Pain?
If you are suffering from chronic pelvic pain, understanding the link between your mind and your body is essential. While "stress" is a word we all use, its biological impact on your pelvic nerves is profound.
At Shree IVF & Endometriosis Clinic, we often see patients with a "clean pelvis"—where all scans and tests come back normal—yet the patient is in genuine, debilitating pain. This is frequently due to how the brain processes hidden emotions and stress.
The Science of "Hidden Drama" and Nerve Endings
Stress isn't just a feeling; it is a physiological signal. Whether it is a missed promotion, an unhappy childhood, or a difficult relationship, these "hidden dramas" pile up in the brain.
When the mind cannot process these emotions, it often lets them out through the nervous system.
Because the pelvis contains a vast majority of the body's nerve endings, it becomes a primary "exit point" for this internal frustration. This triggers a reverse reaction where the nerves become hypersensitive, leading to:
- Vague, localized pelvic pain
- Bloating and digestive discomfort
- Secondary symptoms like headaches and backaches
- Normal test results despite intense physical suffering
A Holistic Path to Pain Relief
When a diagnosis reveals a "clean pelvis," we pivot toward holistic management to desensitize the overactive nerves. This process takes patience, often requiring 3 to 6 months before you feel a tangible difference.
- Sleep Management: Quality sleep is the foundation of nerve recovery. We often prescribe melatonin agonists (like Eunyckta) to help patients achieve deep, restorative sleep, which naturally lowers pain sensitivity.
- Anger and Stress Management: Addressing the root emotional triggers is vital to stopping the "reverse reaction" in the nerves.
- Meditation and Yoga: These techniques are scientifically proven to calm the nervous system and retrain how the brain perceives pain signals.
Why Long-Term Specialist Care is Essential?
Chronic pelvic pain is rarely a "one-fix" situation. It requires chronic management and a doctor who understands the complexity of neuropelvic health.
Many of our patients at Shree IVF & Endometriosis Clinic remain on a follow-up plan for 7 to 10 years. Seeing a specialist like Dr. Jay Mehta ensures that you receive a sensible diagnosis that looks beyond just the physical organs to the health of your entire nervous system.
Taking the Next Step
If you've been suffering from chronic pelvic pain for months or years, seeing multiple doctors without improvement, I encourage you to consult a specialist.
The difference between symptomatic treatment and addressing the root cause can be life-changing.
Remember: your pain is real, your experience is valid, and effective treatment is available. The key is finding the right chronic pelvic pain treatment in India or at a center equipped to provide comprehensive, evidence-based care.
The bottom line: Chronic pelvic pain requires a holistic, specialized approach. Don't settle for years of suffering when expert help is available. Put your head down, find a specialist, and take that crucial step toward diagnosis and relief. Your quality of life is worth it.
Chronic Pelvic Pain Masterclass by Dr. Jay Mehta, India’s Foremost Pelvic Pain Specialist
If you have been told your pelvic pain is "normal" or "all in your head," this masterclass is for you. Chronic pelvic pain is a complex condition that often remains undiagnosed for years because it requires a specialized understanding of the pelvic nervous system.
In this masterclass, Dr. Jay Mehta, a pelvic pain doctor in Mumbai, explains the causes, diagnosis, and advanced treatment options for chronic pelvic pain.
Through these educational videos, you will learn about pelvic nerve disorders, neuropelveology, pelvic nerve mapping, and advanced endometriosis surgery used to treat chronic pelvic pain in women.
Watch the videos below to gain a clear understanding of pelvic pain, why it happens, and the modern treatment options available in India.
FAQs About Chronic Pelvic Pain
- How do I know if my pelvic pain is chronic?
If you have been experiencing pain in your lower abdomen or pelvis weekly for more than six months, and it interferes with your daily activities, it is classified as Chronic Pelvic Pain (CPP).
- Why did my previous ultrasound show a normal pelvis?
Standard ultrasounds are excellent for finding large cysts or fibroids, but they often miss "peritoneal endometriosis." These are flat, tiny implants that require specialized techniques like SonoPODgraphy or a trained chronic pelvic pain specialist to identify.
- Can IBS and pelvic pain be related?
Yes. There is a high overlap between IBS and pelvic pain. Because the nerves supplying the bowel and the reproductive organs are closely linked in the pelvis, inflammation in one can trigger pain in the other.
- What is the difference between interstitial cystitis pelvic pain and endometriosis?
Interstitial cystitis pelvic pain stems from the bladder lining, while endometriosis stems from tissue implants outside the uterus. Both can cause severe pelvic agony and often require a specialist to distinguish between them through clinical examination.
- Is surgery the only option for chronic pelvic pain treatment in women?
Not always. Depending on the diagnosis, we may start with chronic pelvic pain therapy such as hormonal management, pelvic floor physiotherapy, or nerve-calming medications.
However, if fibrosis or nerve impingement is present, surgery is often the most effective way to achieve immediate relief.
Dr. Jay Mehta is a highly renowned IVF specialist and fertility-preserving surgeon based in Mumbai, India. As the director of the Shree IVF and Endometriosis Clinic in Mumbai, he is recognized as one of India's leading laparoscopic gynecologists for advanced treatment of complex conditions such as endometriosis and adenomyosis. Dr. Mehta and his team have extensive expertise, performing more than 2500 endometriosis cases across India every year at multiple locations. Under his leadership, the Shree IVF and Endometriosis Clinic has consequently become the highest-volume endometriosis and adenomyosis treatment unit in India. Dr. Mehta conducts operations and consultations across India's major cities, including Pune, Chennai, Hyderabad, Bangalore, Ahmedabad, Agra, and Delhi. To book an appointment, call: 1800-268-4000
Dr. Jay Mehta
MBBS, DNB – Obstetrics & Gynecology
IVF & Endometriosis Specialist, Laparoscopic Surgeon (Obs & Gyn)

4.9
![]()
Verified & Most Trusted One
Many Treatments. One Goal.
Caring for Every Patient, Every Day.
ALPA AINCHWAR
Thank you to the best endometriosis surgeon in our India.
Honest and very ethical person.
I want to add one thing, very respectful behavior towards all the patients here.
The only thing is doctor jay is very straight forward.
If he is getting so much work being so straight forward. I can only imagine what will happen if he becomes little sweet and sugary sugary to everyone. But whatever I know him he won’t become like that, kyunki iss Bande ko bhagwaan ka kuch alag aashirvaad hai
Vidhi Mehta
Dr Jay Mehta is a genius at treating endometriosis patients. To the point, no bakwaas. For 13 years I was made to believe I could never conceive naturally, from the age of 19 when I went to a hospital for the first time as an emergency endo patient.
After 2 endo surgeries, 1 failed IVF and a miscarriage here I meet the first doctor who said you will conceive naturally. (Hope). , This was God’s plan, Lord Shiva!!
Thank you Dr. Jay, Dr. Vismay, and the entire team for the hope, treatment, hospitality, and the quickest discharge.
RENUKA RAUT
Great Experience. I have been operated for grade 4 endometriosis. I have never seen a doctor like Jay Sir in my entire life..he is very concerned about his patients..going out of the way to make things possible
Finally, I found an endometriosis specialist after struggling a lot. I am In a safe hand. Each and every staff of this hospital is well-trained and well-managed..highly recommended
Sunitha Suni
He is the god me because im suffering from since 4year pain full period of endometriosis problem im going to so many hospitals any one not identify the problem he is identify and clear endometriosis problem, thanq Dr jay metha sir, Dr Chaitali Rao and ur team Good receiving thanq so much sir ur save my life
md Sohail
Dr. Jay Mehta, what a doctor he is ..hats off.
I really wanted to thank from the bottom of my heart to Dr. Jay Mehta and his dedicated and caring team.
We came from Hyderabad and undergone a major surgery. What a guts he has. I highly recommend Dr Jay Mehta for women who needs a cure for Endometriosis.
Huge thanks to Dr. Chaitali, Dr. Vismai sir and all the supporting staff, nurses and mausis. He is the great doctor and do the best treatment.
Overall very rare kind of personality is Dr.Jay Mehta among the present generation of doctors.
Ankit Jain
I wanted to thank Dr. Jay and his dedicated and caring team at Shree IVF & Endometriosis Hospital at Ghatkopar, Mumbai for the Endometriosis surgery performed. His knowledge of this dreadful disease and its treatment to help thousands of endometriotic women is truly amazing.
He is a gem of a person, explains the problem to patients and their families nicely, and proposes surgical treatment. His caring team also makes the stay in the hospital post-op help to recover quickly.
I highly recommend Dr Jay Mehta for women who need a cure for Endometriosis. He also works brilliantly for IVF and other gynac issues. Kindly check with the clinic and hospital and plan your visit accordingly. They also help with nearby stays for outstation patients. God bless you and give you the strength to continue to work in the noble field.
Blogs

Chances of Getting Pregnant with Endometriosis?
Endometriosis doesn’t always mean infertility. Around 70% of women with minimal to moderate stages conceive without fertility treatment

Can Endometriosis Come Back After Surgery?
Endometriosis may return after surgery, as there’s no guaranteed way to stop it completely. But you can take steps to stay aware and support your health.
Videos

Does Endometriosis Affect the Value of the Anti-mullerian Hormone (AMH)?
Yes, endometriosis can impact your AMH level by damaging the ovaries, fallopian tubes, and surrounding pelvic area.

Pain in Endometriosis
Symptoms of endometriosis include period pain, pelvic and back pain, painful sex, leg pain, and bowel discomfort. Pain can be chronic or intense